
Abstract
It is well known that intake of grapefruit juice affects the pharmacokinetics of various kinds of drugs. It has been reported that other citrus juices also interact with certain drugs. To re-evaluate citrus juice-drug interactions based on currently available evidence, a literature search was conducted for new and updated information since the grapefruit juice-drug interaction was last reviewed in 1998. MEDLINE (1998–October 2004) was accessed and more than 200 reports were found. The effects of grapefruit juice ingestion on the pharmacokinetics of orally administered drugs have been reported for 40 drugs since the reviews published in 1998. Increases in either area under the concentration-time curve (AUC) or maximum plasma concentration (Cmax) were found with 34 of these, the major mechanism being considered to be inactivation of intestinal cytochrome P450 3A4, a so-called mechanism-based inhibition. Although recent reports point to the inhibitory effects of grapefruit juice on the function of P-glycoprotein, which transports substrates from enterocytes back into the lumen, the contribution to the bioavailability of drugs that are substrates of P-glycoprotein has not been established yet. Dramatic decreases in AUC and Cmax for two drugs in association with grapefruit juice ingestion has been reported and, in these cases, inhibitory effects on organic anion transporting polypeptide, which mediates absorption from the intestinal lumen to enterocytes, might be involved. Other citrus juices such as Seville (sour) orange juice and commonly ingested varieties of orange juice also showed significant effects on the AUC and Cmax of some drugs. Although the situation is complex and uncertainties remain, we recommend that patients avoid citrus juice intake while taking medications and that healthcare providers advise against citrus juice intake in this setting until any interactions with subject drugs can be clarified in clinical studies.
Similar content being viewed by others
It is generally accepted that intake of some foods may affect the pharmacokinetics of drugs. For example, foods containing many metal ions, such as calcium, magnesium, aluminium, iron (milk, milk products, etc.) inhibit the absorption of some antibacterial agents (tetracycline, enoxacin, etc.) because of chelation. Recently, it was reported that St John’s wort, one of the world’s most popular herbal preparations, can reduce the blood concentrations of some drugs, including warfarin (an anticoagulant), theophylline (a bronchodilator) and oral contraceptives by induction of cytochrome P450 (CYP) 3A4 (the isoform most active in drug metabolism by CYP), CYP2C9, CYP1A2 or P-glycoprotein.[1] Changes in pharmacokinetic parameters, such as area under the concentration-time curve (AUC), maximum plasma concentration (Cmax), time to reach Cmax (Tmax) and elimination half-life (t½) of a drug, resulting from ingestion of combinations of food would depend on the kind and amount of foodstuffs ingested, the drug itself and the timing of administration relative to food intake.
In 1991, the first clinical study of grapefruit juice-drug interaction demonstrated an obvious increase in the AUC and Cmax of the calcium channel antagonists felodipine and nifedipine.[2] Since then, many studies of grapefruit juice-drug interactions have been conducted and two reviews of this topic were published in 1998.[3,4] The major conclusions were that grapefruit juice increases the AUC and Cmax of orally coadministered drugs, such as felodipine, nitrendipine and nisoldipine (calcium channel antagonists), ciclosporin (an immunosuppressant), terfenadine (an antihistamine) and midazolam and triazolam (anxiolytics) and that drugs with lower oral bioavailability are affected to a greater degree. The mechanism of action is considered to be inhibition of CYP3A4 in the small intestine, probably as a result of accelerated CYP3A4 degradation, which means that the process is ‘mechanism-based’ rather than competitive. The effect of grapefruit juice continues for up to 24 hours at least after intake and cumulative effects with time have been observed. On the basis of results from in vitro studies, the candidate ingredients in grapefruit juice that are predicted to account for this interaction are naringin (flavonoid) and 6′,7′-dihydroxybergamottin (furanocoumarin). However, when the reviews were conducted in 1998, the candidates for the causative ingredient were still under investigation because clinical investigations, using pure naringin or supernatant and particle fractions of grapefruit juice suggested that neither of these substances would make a major contribution to interactions in humans.
We conducted a literature search of MEDLINE (1998–October 2004) using the keyword ‘grapefruit juice’ for new and updated information since the subject of grapefruit juice-drug interaction was last reviewed in 1998[3,4] and found more than 200 reports. Therefore, in this article, we re-evaluate grapefruit juice-drug interactions (mechanisms, kinds of drugs affected, extent of effects and active ingredients). Furthermore, because recent reports have shown interactions between other citrus juices and some drugs, we also summarise these new findings, focusing on active ingredients. Finally, we propose recommendations for patients and healthcare providers in relation to the risks of taking medications close to citrus juice ingestion.
1. Mechanism of Grapefruit Juice-Drug Interactions
Two previous reviews showed that grapefruit juice acts at the absorption stage in the small intestine because of the lack of interaction between grapefruit juice and intravenously administered drugs; reduction of intestinal CYP3A4 activity was considered a possible mechanism (see section 1.1).[3,4] In addition to an effect on CYP3A4, new and updated reports have suggested the involvement of two transporters in the small intestine (see sections 1.2 and 1.3).
1.1 Cytochrome P450 3A4
In previous reviews, a mechanism-based inhibition of intestinal CYP3A4 was cited as the cause of grapefruit juice-drug interactions, based on the finding that CYP3A4 protein content in enterocytes (luminal epithelial cells in the small intestine) was reduced without change in corresponding messenger RNA levels after grapefruit juice ingestion in human volunteers.[5] In mechanism-based inhibition, the inhibitor is metabolically activated by an enzyme and then irreversibly inactivates the same enzyme by covalent binding,[6,7] which means that return of enzyme activity requires de novo enzyme synthesis. However, it had been reported in previous reviews[3,4] that some ingredients in grapefruit juice exhibited competitive (reversible) inhibition of CYP3A4 activity in vitro. The relative importance of these two different mechanisms in clinical grapefruit juice-drug interactions has yet to be clarified.
Recently, mechanism-based inhibition was also demonstrated in in vitro experiments using cell free enzyme assay systems[8–10] and in a human colon carcinoma cell line (Caco-2 cells).[11] In addition, two studies of the active ingredients of grapefruit juice[10,12] (see sections 4.1.1 and 4.1.2) have suggested that, rather than competitive inhibition, a mechanism-based inhibition of intestinal CYP3A4 greatly contributes to grapefruit juice-drug interactions in vivo.
1.2 P-Glycoprotein
P-glycoprotein was initially isolated because of its role in multidrug resistance to cancer chemotherapeutic agents. Subsequent studies revealed that this transporter is also involved in the pharmacokinetics of many drugs. P-glycoprotein is expressed in the luminal epithelial cells of tissues that are often associated with drug absorption and disposition, for example, hepatocyte canalicular membrane, renal proximal tubules, the intestinal mucosa and the capillaries of the brain.[13] Therefore, inhibition of P-glycoprotein function at these sites might be expected to increase the oral bioavailability of P-glycoprotein substrate drugs.
An inhibitory effect of grapefruit juice on P-glycoprotein may occur mainly in the intestinal wall because of a lack of grapefruit juice effect on the bioavailability of intravenously administered drugs.[14–17] Recently, in vitro studies using Caco-2 cells have clearly shown an inhibitory effect of grapefruit juice on efflux of substrates of P-glycoprotein.[18,19] Because P-glycoprotein and CYP3A4 share many substrates and inhibitors,[20] inhibition of P-glycoprotein function is speculated to augment the grapefruit juice-drug interaction resulting from CYP3A4 inhibition.[20] For example, although ciclosporin is known to be a substrate of both intestinal CYP3A4 and P-glycoprotein, a more significant contribution of intestinal P-glycoprotein to the oral bioavailability of this drug has been demonstrated in kidney transplanted patients.[21] Grapefruit juice was reported to increase the oral bioavailability of ciclosporin (AUC increased by a maximum 40–60%), probably by inhibition of P-glycoprotein because Seville (sour) orange juice (see section 3.2) significantly reduced enterocyte concentrations of CYP3A4 with no influence on ciclosporin disposition.[22] On the other hand, other studies found that the pharmacokinetic parameters of digoxin (a cardiotonic agent) were not affected[23] or only slightly and not significantly affected by grapefruit juice ingestion in healthy volunteers (1.2-fold and 1.1-fold increase in AUC and Cmax, respectively ).[24] However, although digoxin is a substrate for P-glycoprotein that is minimally metabolised, it is not considered an appropriate probe for evaluating the clinical effect of grapefruit juice on intestinal P-glycoprotein because of its high oral bioavailability (70–80%).[25,26] There is no other information available on the effects of grapefruit juice ingestion on P-glycoprotein function in vivo.
1.3 Organic Anion Transporting Polypeptide
Recently, marked reduction of both the AUC and Cmax of fexofenadine (an antihistamine) and celiprolol (a β1-adrenoceptor antagonist) by grapefruit juice was reported.[27,28] These studies provided the first indications that the oral bioavailability of drugs can be dramatically reduced by grapefruit juice ingestion. Because both fexofenadine and celiprolol are not metabolised by CYP3A4 but are substrates of P-glycoprotein, it had been expected that their bioavailability would have been increased by grapefruit juice ingestion. Therefore, the involvement of a third mechanism in the interaction between grapefruit juice and drugs has been suggested.
Dresser et al.[27] focused on one intestinal transporter, the organic anion transporting polypeptide (OATP), which assists uptake of drugs on the luminal side of enterocytes, thereby opposing the function of P-glycoprotein. These investigators revealed that grapefruit juice markedly reduces human OATP function in vitro at a concentration of 0.5%, while P-glycoprotein function is only slightly and not significantly inhibited even at the 10-fold higher concentration of 5.0%. It is considered that this more potent effect of grapefruit juice on OATP function is responsible for the reduction in the AUC and Cmax of fexofenadine and celiprolol reported in the previously mentioned clinical studies.[27,28] Based on these findings, Dresser et al.[29] proposed a new model involving OATP for fruit juice-drug interaction in small intestine enterocytes.
2. Effects of Grapefruit Juice on the Concentration-Time Curve and Maximum Concentration of Drugs
Tables I, II and III summarise results for all drugs for which pharmacokinetic clinical studies have reported on grapefruit juice-drug interactions; some previously reviewed data are also included in these tables. Although orange juice was used as a control in some studies as shown in section 3.1, the results of these studies were deleted as much as possible because of reports of interactions between orange juice and drugs (see section 3.1). Since the 1998 reviews,[3,4] 37 drugs have been newly found to interact with grapefruit juice in clinical trials. Most studies were conducted by cross-over design and used approximately ten healthy volunteers, but the amount/concentration of ingested grapefruit juice, the frequency of administration and the timing relative to drug administration were variable. The extent of change in the AUC and Cmax also varied with different drugs. On the basis of changes in AUC and Cmax, drugs could be classified into the following three groups: group 1: increase (>30% increase in either AUC or Cmax) ; group 2: no change; and group 3: decrease (>20% decrease in either AUC or Cmax).


Increases in area under the concentration-time curve (AUC) and maximum plasma concentration (Cmax) with grapefruit juice for group 1 drugs (i.e. drugs with >30% increase in either AUC or Cmax). Data with maximum change in AUC are shown


Primary metabolic enzyme and oral bioavailability of group 2 drugs (i.e. drugs with no change in area under the concentration-time curve [AUC] or maximum plasma concentration [Cmax] with grapefruit juice)

Decreases in AUC and Cmax with grapefruit juice for group 3 drugs (i.e. drugs with >20% decrease in either AUC or Cmax). Data with maximum change in AUC are shown
2.1 Group 1 Drugs
In table I, increases in the AUC and Cmax of 34 drugs interacting with grapefruit juice are listed in ascending order of oral bioavailability. Most of these drugs are substrates of CYP3A4. Although the degree of increase in AUC and Cmax appeared to be reciprocal with the value of bioavailability after oral administration (as in previous reviews), this was not always the case. The major reason for this discrepancy is likely to be related to the degree of first-pass metabolism in the intestinal wall. Differences in the method of grapefruit juice ingestion among clinical studies might also be a factor. However, since some drugs such as diazepam and methylprednisolone showed a greater change in AUC than the maximum expected from the bioavailability, elimination of these drugs from the blood might be reduced by grapefruit juice ingestion although there is no supporting evidence for this at present. Thus, the clinical risk levels associated with taking particular drugs in combination with grapefruit juice are not easily estimated because the extent of increase in AUC and Cmax is variable and the actual effects would depend on the pharmacological activity of the parent drug/metabolite, the drug’s safety margin and the type of adverse effects the drug causes. Furthermore, it should be mentioned that most clinical studies were conducted for only short periods and involved small numbers of healthy volunteers, rather than over the long-term with patients requiring drug therapy.
New and/or updated information on the pharmacokinetic and pharmacodynamic changes of group 1 drugs with grapefruit juice ingestion are presented in the following sections.
2.1.1 Buspirone
Buspirone is an anxiolytic agent with an oral bioavailability of only 4%.[87] Because a potent CYP3A4 inhibitor, itraconazole, has been shown to greatly increase the AUC of buspirone,[88] it is considered to be metabolised by this enzyme. Grapefruit juice increased the AUC of buspirone 9.2-fold and the Cmax 4.2-fold, but a significant increase in pharmacodynamic effects was seen only in relation to subjective overall drug effect.[32] The relatively modest impact of grapefruit juice on buspirone may be explained at least in part by the fact that the intensity of a drug effect is generally proportional to the logarithm of the drug concentration in blood.
2.1.2 HMG-CoA Reductase Inhibitors
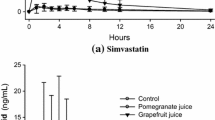
Simvastatin, lovastatin and atorvastatin have HMG-CoA reductase inhibitory activity that results in reductions in cholesterol biosynthesis. Rhabdomyolysis is known as a rare but severe adverse effect of these agents.[89] They are metabolised by CYP3A4 and have low oral bioavailability (12% for atorvastatin and ≤5% for simvastatin and lovastatin).[89] A battery of clinical studies[33,34,42] that included intakes of large quantities of grapefruit juice (200mL double-strength grapefruit juice intake three times daily for 3 days and drug administration with the first intake of grapefruit juice on the third day), showed a marked increase in AUC for simvastatin and lovastatin (>10-fold). However, HMG-CoA reductase inhibitory activity increased only 3.6-fold for simvastatin. Although the AUC for atorvastatin increased 2.5-fold, the AUC values for its major metabolites following CYP3A4 metabolism decreased by 15–26%. Because the metabolites of atorvastatin have significant HMG-CoA reductase inhibitory activity, this decrease in the AUC of the metabolites of atorvastatin might lead to a lesser increase in the total activity in blood (1.5-fold for atorvastatin) than might be expected by consideration of the AUC for the atorvastatin. Therefore, the clinical risk arising from concomitant use of grapefruit juice and these drugs is not as large as would be expected from the change in pharmacokinetic parameters of the parent drugs. In other studies, conducted under more actual conditions, it was reported that the AUC of lovastatin increased 1.94-fold (oral dose of lovastatin in the evening after consuming an 8-ounce glass of regular-strength grapefruit juice with breakfast for 3 days),[90] and that of atorvastatin increased 1.40-fold (200mL regular-strength grapefruit juice intake three times daily for 3 days and drug administration with the first intake of grapefruit juice on the third day).[81]
2.1.3 Dextromethorphan
Although there is no information available on the oral bioavailability in humans of dextromethorphan, an over-the-counter and prescribed antitussive agent, it is a substrate of CYP3A4 and CYP2D6. Grapefruit juice increased the bioavailability of dextromethorphan by 5.4-fold, based on analysis of the compound and its metabolites in urinary samples.[41] However, the interaction between grapefruit juice and dextromethorphan would not be as clinically important as expected because metabolites are reported to have the same extent of pharmacodynamic activity as the parent drug.[91]
2.1.4 Amiodarone
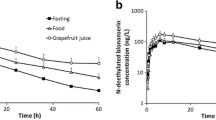
Amiodarone, an antiarrhythmic agent, is metabolised by CYP3A4 to the more potent metabolite N-desethylamiodarone. The oral bioavailability of the parent drug is 67%.[89] Administration of amiodarone is known to cause torsade de pointes, a rare but sometimes fatal ventricular arrhythmia, which occurs in the context of QT interval prolongation.[89] This is one of the most serious clinical risks associated with group 1 drugs. Grapefruit juice completely inhibited the production of N-desethylamiodarone, resulting in 50% and 84% increases in the AUC and Cmax of amiodarone, respectively.[54] As expected from experimental results showing greater electrophysiological properties of N-desethylamiodarone than those of the parent drug,[92,93] the pharmacodynamic effect (QT prolongation) of concomitant use of grapefruit juice is smaller than that expected from pharmacokinetic studies. In a clinical study, grapefruit juice reduced the prolongation in QT intervals caused by the administration of amiodarone.[54]
2.1.5 Antimalarial Agents
Interactions between antimalarial agents and grapefruit juice have been newly reported since the reviews published in 1998.[3,4] The oral bioavailability of artemether could not be estimated because intravenous administration has not been approved for this agent. Grapefruit juice increased the AUC and Cmax of artemether by 3.5-fold and 2.6-fold, respectively,[60] but there is no information on pharmacodynamic changes. For halofantrine, torsade de pointes is one of the known adverse effects.[89] With grapefruit juice, a 2- to 3-fold increase in the extent of QT interval prolongation was reported with 2.8-fold and 3.2-fold increases in the AUC and Cmax of this drug, respectively.[40] Because of concerns about the risk of torsade de pointes, concomitant use of grapefruit juice with halofantrine should be avoided.
2.1.6 Ciclosporin
Ciclosporin, an immunosuppressant, is used in transplant patients and is a substrate of CYP3A4 and P-glycoprotein. It is well known that grapefruit juice significantly increases the AUC and Cmax of orally administered ciclosporin in renal transplant patients and healthy volunteers, although the extent of these increases is only 40–60% (maximum).[17] Recent reports have provided similar results and shown that grapefruit juice also affects the formation and/or elimination of metabolites M1 and M9.[94-96] Although changes in the AUC and Cmax of the M1 metabolite were equivocal, reductions in the AUC and Cmax for the M9 metabolite were consistently observed. The increased systemic exposure to ciclosporin and changes in its metabolites might suggest that metabolic inhibition of ciclosporin by intestinal CYP3A4 could occur in combination with grapefruit juice. However, the major contribution to the increase in the AUC and Cmax of ciclosporin by grapefruit juice is considered to result from a reduction in P-glycoprotein function (see section 1.2). Although the inhibitory effect of grapefruit juice on P-glycoprotein has clearly been shown in vitro (see section 1.2), the change in the AUC of ciclosporin is moderate.[17] However, the consequent effect would not be negligible because of high individual differences in bioavailability, the potential for serious adverse effects (nephrotoxicity, hypertension and cerebral toxicity) and the narrow therapeutic index of ciclosporin.[89]
2.2 Group 2 Drugs
Table II lists 19 drugs for which both the AUC and Cmax appear not to be affected in combination with grapefruit juice ingestion, together with the primary metabolic enzymes involved with metabolism of these drugs and their oral bioavailabilities. For most drugs in this group, the results of clinical studies are newly reported. The pharmacokinetic parameters of alprazolam (an anxiolytic agent), quinine (an antimalarial agent), quinidine (an antiarrhythmic agent), indinavir (an anti-HIV protease inhibitor), clarithromycin (an antibacterial agent) and amlodipine (a calcium channel antagonist) were not affected by grapefruit juice despite the fact that their primary metabolic enzyme is CYP3A4. Therefore, it is considered that the primary metabolism of these drugs might not occur in the small intestine. The other drugs listed in table II are not metabolised by CYP3A4 or are metabolised by both CYP3A4 and other enzymes. For example, the pharmacokinetic parameters of losartan were barely affected by the CYP3A4 inhibitor itraconazole because losartan is a substrate for both CYP3A4 and CYP2C9.[97,98]
2.3 Group 3 Drugs
Recently, some clinical studies have shown that concomitant intake of grapefruit juice can decrease the AUC and Cmax of orally coadministered drugs (table III).
For example, values for fexofenadine and celiprolol were markedly lowered when coadministered with grapefruit juice. For fexofenadine, a concentration relationship was detected, i.e. 100% grapefruit juice decreased AUC by approximately 70% whereas 25% diluted grapefruit juice decreased AUC by approximately 20%.[27] Since the metabolism of fexofenadine and celiprolol is negligible in humans[99] and the amounts of drug excreted in urine was reduced without decreasing renal clearance, grapefruit juice was considered to inhibit the absorption of these drugs.[27,28] A possible mechanism is inhibition of uptake via OATP (see section 1.3). Fexofenadine is known to be a substrate of OATP, but there is no relevant information with regard to celiprolol. Other mechanisms, such as changes in intraduodenal pH and formation of complexes between drugs and components of grapefruit juice, cannot be discounted.
Itraconazole, an antifungal agent, is metabolised by CYP3A4 to hydroxyitraconazole. Concomitant intake of double-strength grapefruit juice with itraconazole capsules caused decreases in the AUC values for both itraconazole and hydroxyitraconazole of approximately 50%, but the metabolic ratio (hydroxyitraconazole AUC vs itraconazole AUC) was not affected, suggesting that there was no influence on itraconazole metabolism.[83] The investigators proposed that a decrease in duodenal pH or delay in gastric emptying by grapefruit juice would result in decreased itraconazole absorption. Involvement of OATP is also likely, although there is no actual evidence of this. Contrary to the findings reported in the above-mentioned study,[83] a recent study conducted by Gubbins et al.[100] showed a slight but significant increase (1.2-fold) in itraconazole AUC with grapefruit juice. This study evaluated the interaction between an oral solution of itraconazole formulated in hydroxypropyl-β-cyclodextrin and a different grapefruit juice schedule (ingestion of 240mL of single-strength grapefruit juice three times daily for 2 days). The investigators noted the differences in volume, viscosity and caloric density of the grapefruit juice preparation compared with standard regimens and further studies are needed.
It should be taken into account that the decrease in AUC and/or Cmax of group 3 drugs caused by grapefruit juice interaction may lessen their pharmacological effects. Particularly in the case of celiprolol, which is indicated for hypertension, great care would need to be taken because the decrease in AUC and Cmax could lead to a sharp rise in blood pressure. Although grapefruit juice effects on the pharmacokinetics of amprenavir, etoposide and theophylline are small, caution should also be taken with use of these drugs because of their narrow therapeutic range.
2.3.1 Discussion
Although the variability (individual differences) in clinical studies listed in the tables is generally high, this is dependent on the drugs studied. Therefore, it should be noted that small changes in average AUC and Cmax do not always translate into a negligible effect in all individuals; very high individual differences in the bioavailability of ciclosporin, for example, can be observed. When focusing on how any particular drug is affected by grapefruit juice, the variability in the original report should be checked to obtain a true clinical perspective. The potential for different responses in sensitive subpopulations is another important issue. For example, a grapefruit-felodipine interaction study in elderly individuals showed greater increases (AUC 2.9-fold, Cmax 4.0-fold)[101] than those reported in clinical studies that have mostly involved healthy young volunteers. Thus, the elderly should be particularly cautioned about concomitant ingestion of grapefruit juice with drugs.
From a different point of view, Bailey[89] has suggested that there are potential beneficial effects with concomitant ingestion of grapefruit juice, such as enhanced drug efficacy. As autoinduction of CYPs is a concern for CYP-metabolised drug therapy, grapefruit juice could be useful in the maintenance of drug effectiveness. However, because grapefruit is a natural product and the ingredient and mechanism of action responsible for its effects are not yet fully understood, it is difficult to recommend grapefruit juice as a booster. Another possible countermeasure is the substitution of grapefruit juice sensitive agents (group 1 drugs) for grapefruit juice tolerant agents (group 2 drugs) in the same therapeutic classes.[102] However, it should be noted that each drug has different characteristics, such as absorption, distribution, metabolism and excretion.
3. Interactions Between Other Citrus Juices and Drugs
Recently, some reports have been published regarding interactions between citrus juices other than grapefruit juice and drugs.
3.1 Orange Juice (Sweet)
In the first clinical study of grapefruit juice and drug interaction,[2] it became clear that orange juice, in contrast, did not affect the pharmacokinetics of felodipine. Subsequently, orange juice was sometimes used as a negative control in studies of grapefruit juice-drug interactions. However, notable clinical results that might reverse this long-held stance have recently been reported. In one study, orange juice reduced the AUC and Cmax of fexofenadine by up to 30%, an effect similar to that of grapefruit juice.[27] Orange juice also substantially reduced the Cmax, AUC and urinary excretion of celiprolol by 89%, 83% and 77%, respectively.[103] An in vitro study showed that orange juice has a much stronger inhibitory effect on OATP than P-glycoprotein,[27] so it would be expected to inhibit OATP-mediated transport rather than P-glycoprotein function in vivo. Unexpectedly, apple juice, a non-citrus juice, was also reported to have the same effect on fexofenadine in vivo and OATP-mediated transport in vitro.[27]
3.2 Seville (Sour) Orange Juice
Seville (sour) orange is mainly used for confectionary products such as marmalade. Although its juice is not fit to drink because of its sour taste, several interaction studies with Seville (sour) orange juice have been conducted. The increase in the AUC of felodipine, a CYP3A4 substrate, with Seville (sour) orange juice is the same as that observed with diluted grapefruit juice; both juice preparations contained the same total concentrations of candidate causative ingredients bergamottin plus 6′,7′-dihydroxybergamottin.[104] A significant increase in the oral bioavailability of dextromethorphan with Seville (sour) orange juice has also been reported.[41] Because it has been reported that Seville orange juice decreases the enterocyte concentration of CYP3A4,[22] mechanism-based inhibition must be considered. The lack of interaction between Seville (sour) orange juice and ciclosporin[22] suggests that Seville orange juice does not inhibit intestinal P-glycoprotein function.
3.3 Other Citrus Juices
The juice of another citrus, the tangerine (a kind of Mandarin orange), has been reported to decrease the AUC of midazolam (an anxiolytic) by about 40% over the first 1.5 hours and to increase Tmax 2-fold without effects on total AUC, Cmax and the AUC ratio of the main metabolite to midazolam.[105] Tangerine juice might have some impact on the absorption process of midazolam.
Lime juice has demonstrated mechanism-based inhibition of CYP3A4 activity in vitro.[10] However, in a clinical study, 25% diluted lime juice containing the candidate causative ingredient bergamottin in the same amounts as grapefruit juice (see section 4.1.2), did not exert any significant effects on the pharmacokinetic parameters of felodipine.[10]
To our knowledge, there is no further information available on interactions between drugs and tangerine or lime juice.
3.4 Target Sites of Citrus-Drug Interaction in Enterocytes
Both P-glycoprotein and OATP as well as CYP3A4 are expressed in the liver and their involvement in drug disposition and exclusion has been reported.[106–108] However, the lack of interaction between grapefruit juice and intravenously administered drugs[1,6,14,15,17] suggests that hepatic enzymes and transporters are minimally, if at all, involved. Based on the findings mentioned in sections 1, 3.1 and 3.2 and the new model proposed by Dresser and Bailey,[29] we describe the target sites in small intestine enterocytes where various citrus juices exert their inhibitory actions (figure 1).

The target sites in enterocytes of the small intestine for various citrus juices. CYP3A4 = cytochrome P450 3A4; OATP = organic anion transporting polypeptide.
If drugs are substrates of CYP3A4, they will be partially metabolised in the intestine and their metabolites will appear in the portal vein. Drugs that are substrates of OATP will be absorbed into enterocytes with the aid of OATP and passed through to the portal vein. Drugs that are substrates of P-glycoprotein may be transported back into the small intestine.
Grapefruit juice inactivates CYP3A4 in a mechanism-based manner and inhibits the function of P-glycoprotein and OATP. It appears that orange juice has inhibitory effects on P-glycoprotein and OATP, but not on CYP3A4. The effects of grapefruit juice and orange juice on P-glycoprotein are likely to be weak. Seville (sour) orange juice is considered to inactivate CYP3A4 by a mechanism-based action, but not to inhibit the function of P-glycoprotein. Possible effects of Seville (sour) orange juice on OATP remain to be elucidated.
4. Causative Ingredients
Several hundred ingredients have been identified in grapefruit juice.[109] The composition of the juice varies widely, depending on the genetic background of the plant, environmental conditions during fruit growth, fruit maturity and fruit processing.[109,110] Although several studies have been conducted, definite conclusions as to causative ingredients cannot be drawn yet.
4.1 Candidate Ingredients for CYP3A4 Inhibition
Flavonoids and furanocoumarins, which are found in grapefruit juice and Seville (sour) orange juice but not in orange juice, have been proposed as causative ingredients of CYP3A4 inhibition by grapefruit juice.
4.1.1 Flavonoids
Naringin (naringenin glycoside) is the most prevalent flavonoid in grapefruit juice.[111] Although naringin is hydrolysed by intestinal bacteria to naringenin[112,113] (figure 2), which has CYP3A4 inhibitory activity in vitro,[3,4] clinical studies using commercially-available pure naringin have shown that it is not the major inhibitory ingredient of grapefruit juice.[114–116] Recently, naringenin was reported to cause competitive, but not mechanism-based, inhibition of CYP3A4 activity in vitro,[12] but such competitive inhibition is known to be not important for the clinical grapefruit juice-drug interaction.[89]

Chemical structures of (a) naringin and (b) naringenin.
4.1.2 Furanocoumarins
The furanocoumarins exert mechanism-based inhibition of CYP3A4 in vitro,[9] but clinical studies using pure forms cannot be conducted because these have not yet been approved for human intake. Previously, although 6′,7′-dihydroxybergamottin (figure 3), one of the most abundant furanocoumarins, was proposed as an active ingredient in grapefruit juice, subsequent clinical studies using supernatant and particulate fractions obtained by means of centrifugation and filtration of grapefruit juice showed that 6′,7′-dihydroxybergamottin was not the major active ingredient.[117]

Chemical structures of (a) bergamottin and (b) 6′,7′-dihydroxybergamottin.
Information on bergamottin (figure 3), another major furanocoumarin, has been newly reported. Guo et al.[9] showed that bergamottin and some other furanocoumarins concentrated by centrifugation in the particulate fraction increased felodipine AUC 1.4 times more than the supernatant fraction in the above-mentioned clinical study.[117] Furthermore, Bailey et al.[12] reported that an extract of segment-free parts of grapefruit, which included more bergamottin and less 6′,7′-dihydroxybergamottin, increased felodipine AUC considerably more than the segments, again suggesting that bergamottin might be the major inhibitory component in grapefruit juice. However, diluted lime juice containing bergamottin in the same quantity as in grapefruit juice, but free from 6′,7′-dihydroxybergamottin, could only partially reproduce the effect of grapefruit juice on felodipine AUC and the investigators concluded that bergamottin was not a primary substance responsible for clinical inhibition of CYP3A4 activity.[10] Recently, however, findings from a study of furanocoumarin fractions of grapefruit diluted in orange juice supported the notion that 6′,7′-dihydroxybergamottin contributes to the grapefruit juice-felodipine interaction.[118]
Bergapten is another ingredient found in grapefruit juice preparations according to one study,[119] although other investigators deny its existence.[104] Bergapten is also found in Seville (sour) orange juice.[9] Bergapten’s mechanism-based inhibition of CYP3A4 has been shown in vitro, albeit with only about one-third of the potency of that reported for 6′,7′-dihydroxybergamottin.[104] However, as one grapefruit juice preparation that had no detectable levels of bergapten significantly increased the AUC and Cmax of felodipine,[104] bergapten is unlikely to be a major active ingredient in grapefruit juice-drug interactions.
Another bergamottin derivative, epoxybergamottin, has been reported to be present in grapefruit juice in only minor quantities.[9] Epoxybergamottin has also demonstrated mechanism-based inhibition of CYP3A4 in vitro,[12] but it is not chemically stable and is considered to be rapidly converted to 6′,7′-dihydroxybergamottin in the gastrointestinal tract.
Two dimers of furanocoumarins, GF-I-1Footnote 1 and GF-I-4Footnote 2, are minor components in grapefruit juice. They are reported to reduce CYP3A4 activities through both competitive and mechanism-based inhibition over 100 times more potently than 6′,7′-dihydroxybergamottin or bergamottin in vitro,[9,120] but further information on these two dimers, including clinical data, are unfortunately lacking.
Given the available data on flavonoids and furanocoumarins and the fact that the contents of the various individual species obviously differ among grapefruit juices,[9] it is possible that the combined effects of all forms of furanocoumarins acting together might contribute to the mechanism-based inhibition of intestinal CYP3A4 in vivo. There is also a possibility that other furanocoumarins could be newly identified as causative agents.
4.2 Candidate Ingredients for P-Glycoprotein Inhibition
Although naringin and naringenin have been shown to inhibit the transport of P-glycoprotein substrates in vitro,[18,27,121] there is insufficient information available to evaluate whether these flavonoids are the main inhibitory ingredients in grapefruit juice. It should be borne in mind that these substances are not present in orange juice, which does have inhibitory effects on P-glycoprotein function.[111]
Some furanocoumarins, such as 6′,7′-dihydroxybergamottin, bergamottin and bergapten, have also been shown to inhibit transport of P-glycoprotein substrates in vitro.[27,119,121,122] However, this might not be relevant in vivo because in vitro data suggest that the major effect of 6′,7′-dihydroxybergamottin is attributable to inhibition of CYP3A4[121] and furanocoumarins are also present in Seville (sour) orange juice,[9] which is considered not to affect the function of P-glycoprotein.
In vitro studies employing fractionation of grapefruit juice suggest that the major P-glycoprotein inhibitors may be different from the major CYP3A4 inhibitors.[18,119] Polymethoxyflavones such as noblletin, heptamethoxyflavone and tangeretine, which are ingredients in orange juice, have been reported to inhibit the function of P-glycoprotein in vitro.[122,123] These compounds are also found in grapefruit juice in lower levels than in orange juice[124] and are known not to inhibit CYP3A4 in vitro.[123]
5. Conclusions
Since the effects of grapefruit juice on 19 drugs were reported in two reviews published in 1998,[3,4] 25 different drugs whose AUC and Cmax are influenced by grapefruit juice have been newly reported. The outcomes in most cases were increases in these parameters, but decreases were reported for six drugs. The increases in AUC or Cmax were probably due to mechanism-based inactivation of intestinal CYP3A4, with a possible minor contribution from decreased P-glycoprotein function; the decreases in AUC or Cmax may have been due to inhibition of intestinal OATP. Other citrus juices, such as Seville (sour) orange juice and orange juice (sweet), have also been found to exert inhibitory effects. However, no specific ingredients in citrus juice have yet been established to have effects on AUC and Cmax in vivo, although furanocoumarins are considered to be the most likely candidates.
Given the complexity of citrus juice-drug interactions and the wide range of drugs affected, we recommend that patients and healthcare providers avoid any citrus juice intake when taking medications until adverse effects due to possible interactions have been ruled out in clinical studies.
Furthermore, since the effect of grapefruit juice on intestinal CYP3A4 is known to continue for more than 24 hours, it might also be necessary to caution against citrus juice intake for at least 1 day before medication is taken. Furthermore, the elderly should be carefully cautioned about the need to avoid concomitant intake of grapefruit juice.
Notes
GF-I-1 (4-[[6-hydroxy-7-[[1-[(1-hydroxy-1-methyl)ethyl]-4-methyl-6-(7-oxo-7{itH}-furo[3,2-g][1]benzopyran-4-yl)-4-hexenyl]oxy]-3,7-dimethyl-2-octenyl]oxy]-7{itH}-furo[3,2-g][1]benzopyran-7-one)
GF-I-4 (4-[[6-hydroxy-7-[[4-methyl-1-(1-methylethenyl)-6-(7-oxo-7{itH}-furo[3,2-g][1]benzopyran-4-yl)-4-hexenyl]-xy]3,7-dimethyl-2-octenyl]xy]7{itH}-furo[3,2-g][1]benzopyran-7-one)
References
Henderson L, Yue QY, Bergquist C, et al. St John’s wort (Hypericum perforatum): drug interactions and clinical outcomes. Br J Clin Pharmacol 2002; 54: 349–56
Bailey DG, Spence JD, Munoz C, et al. Interaction of citrus juices with felodipine and nifedipine. Lancet 1991; 337: 268–9
Bailey DG, Malcolm J, Arnold O, et al. Grapefruit juice-drug interactions. Br J Clin Pharmacol 1998; 46: 101–10
Fuhr U. Drug interactions with grapefruit juice: extent, probable mechanism and clinical relevance. Drug Saf 1998; 18: 251–72
Lown KS, Bailey DG, Fontana RJ, et al. Grapefruit juice increases felodipine oral availability in humans by decreasing intestinal CYP3A protein expression. J Clin Invest 1997; 99: 2545–53
Silverman RB. Mechanism-based enzyme inactivation: chemistry and enzymology. Vol. 1. Boca Raton (FL): CRC Press, 1988: 224
Silverman RB. Mechanism-based enzyme inactivation: chemistry and enzymology. Vol. 2. Boca Raton (FL): CRC Press, 1988: 288
Chan WK, Nguyen LT, Miller VP, et al. Mechanism-based inactivation of human cytochrome P450 3A4 by grapefruit juice and red wine. Life Sci 1998; 62: PL135–42
Guo LQ, Fukuda K, Ohta T, et al. Role of furanocoumarin derivatives on grapefruit juice-mediated inhibition of human CYP3A activity. Drug Metab Dispos 2000; 28: 766–71
Bailey DG, Dresser GK, Bend JR. Bergamottin, lime juice, and red wine as inhibitors of cytochrome P450 3A4 activity: comparison with grapefruit juice. Clin Pharmacol Ther 2003; 73: 529–37
Schmiedlin Ren P, Edwards DJ, Fitzsimmons ME, et al. Mechanisms of enhanced oral availability of CYP3A4 substrates by grapefruit constituents: decreased enterocyte CYP3A4 concentration and mechanism-based inactivation by furanocoumarins. Drug Metab Dispos 1997; 25: 1228–33
Bailey DG, Dresser GK, Kreeft JH, et al. Grapefruit-felodipine interaction: effect of unprocessed fruit and probable active ingredients. Clin Pharmacol Ther 2000; 68: 468–77
Silverman JA. Multidrug-resistance transporters. Pharm Biotechnol 1999; 12: 353–86
Rashid TJ, Martin U, Clarke H, et al. Factors affecting the absolute bioavailability of nifedipine. Br J Clin Pharmacol 1995; 40: 51–8
Kupferschmidt HH, Fattinger KE, Ha HR, et al. Grapefruit juice enhances the bioavailability of the HIV protease inhibitor saquinavir in man. Br J Clin Pharmacol 1998; 45: 355–9
Kupferschmidt HH, Ha HR, Ziegler WH, et al. Interaction between grapefruit juice and midazolam in humans. Clin Pharmacol Ther 1995; 58: 20–8
Ducharme MP, Warbasse LH, Edwards DJ. Disposition of intravenous and oral cyclosporine after administration with grapefruit juice. Clin Pharmacol Ther 1995; 57: 485–91
Takanaga H, Ohnishi A, Matsuo H, et al. Inhibition of vinblastine efflux mediated by P-glycoprotein by grapefruit juice components in caco-2 cells. Biol Pharm Bull 1998; 21: 1062–6
Xu J, Go ML, Lim LY. Modulation of digoxin transport across Caco-2 cell monolayers by citrus fruit juices: lime, lemon, grapefruit, and pummelo. Pharm Res 2003; 20: 169–76
Lin JH, Yamazaki M. Role of P-glycoprotein in pharmacokinetics: clinical implications. Clin Pharmacokinet 2003; 42: 59–98
Lown KS, Mayo RR, Leichtman AB, et al. Role of intestinal Pglycoprotein (mdr1) in interpatient variation in the oral bioavailability of cyclosporine. Clin Pharmacol Ther 1997; 62: 248–60
Edwards DJ, Fitzsimmons ME, Schuetz EG, et al. 6′,7′-dihydroxybergamottin in grapefruit juice and Seville orange juice: effects on cyclosporine disposition, enterocyte CYP3A4, and P-glycoprotein. Clin Pharmacol Ther 1999; 65: 237–44
Parker RB, Yates CR, Soberman JE, et al. Effects of grapefruit juice on intestinal P-glycoprotein: evaluation using digoxin in humans. Pharmacotherapy 2003; 23: 979–87
Becquemont L, Verstuyft C, Kerb R, et al. Effect of grapefruit juice on digoxin pharmacokinetics in humans. Clin Pharmacol Ther 2001; 70: 311–6
Beveridge T, Nuesch E, Ohnhaus EE. Absolute bioavailability of digoxin tablets. Arzneimittel Forschung 1978; 28: 701–3
Cohen AF, Kroon R, Schoemaker HC, et al. The bioavailability of digoxin from three oral formulations measured by a specific h.p.l.c. assay. Br J Clin Pharmacol 1993; 35: 136–42
Dresser GK, Bailey DG, Leake BF, et al. Fruit juices inhibit organic anion transporting polypeptide-mediated drug uptake to decrease the oral availability of fexofenadine. Clin Pharmacol Ther 2002; 71: 11–20
Lilja JJ, Backman JT, Laitila J, et al. Itraconazole increases but grapefruit juice greatly decreases plasma concentrations of celiprolol. Clin Pharmacol Ther 2003; 73: 192–8
Dresser GK, Bailey DG. The effects of fruit juices on drug disposition: a new model for drug interactions. Eur J Clin Invest 2003; 33Suppl. 2: 10–6
Clifford CP, Adams DA, Murray S, et al. The cardiac effects of terfenadine after inhibition of its metabolism by grapefruit juice. Eur J Clin Pharmacol 1997; 52: 311–5
Ebert U, Oertel R, Kirch W. Influence of grapefruit juice on scopolamine pharmacokinetics and pharmacodynamics in healthy male and female subjects. Int J Clin Pharmacol Ther 2000; 38: 523–31
Lilja JJ, Kivisto KT, Backman JT, et al. Grapefruit juice substantially increases plasma concentrations of buspirone. Clin Pharmacol Ther 1998; 64: 655–60
Lilja JJ, Kivisto KT, Neuvonen PJ. Grapefruit juice-simvastatin interaction: effect on serum concentrations of simvastatin, simvastatin acid, and HMG-CoA reductase inhibitors. Clin Pharmacol Ther 1998; 64: 477–83
Kantola T, Kivisto KT, Neuvonen PJ. Grapefruit juice greatly increases serum concentrations of lovastatin and lovastatin acid. Clin Pharmacol Ther 1998; 63: 397–402
Schubert W, Cullberg G, Edgar B, et al. Inhibition of 17 beta-estradiol metabolism by grapefruit juice in ovariectomized women. Maturitas 1994; 20: 155–63
Takanaga H, Ohnishi A, Murakami H, et al. Relationship between time after intake of grapefruit juice and the effect on pharmacokinetics and pharmacodynamics of nisoldipine in healthy subjects. Clin Pharmacol Ther 2000; 67: 201–14
Fuhr U, Maier Bruggemann A, Blume H, et al. Grapefruit juice increases oral nimodipine bioavailability. Int J Clin Pharmacol Ther 1998; 36: 126–32
Soons PA, Vogels BA, Roosemalen MC, et al. Grapefruit juice and cimetidine inhibit stereoselective metabolism of nitrendipine in humans. Clin Pharmacol Ther 1991; 50: 394–403
Fingerova H, Oborna I, Petrova P, et al. Does grapefruit juice increase the bioavailability of orally administered sex steroids? [in Czech]. Ceska Gynekol 2003; 68: 117–21
Charbit B, Becquemont L, Lepere B, et al. Pharmacokinetic and pharmacodynamic interaction between grapefruit juice and halofantrine. Clin Pharmacol Ther 2002; 72: 514–23
Di Marco MP, Edwards DJ, Wainer IW, et al. The effect of grapefruit juice and seville orange juice on the pharmacokinetics of dextromethorphan: the role of gut CYP3A and P-glycoprotein. Life Sci 2002; 71: 1149–60
Lilja JJ, Kivisto KT, Neuvonen PJ. Grapefruit juice increases serum concentrations of atorvastatin and has no effect on pravastatin. Clin Pharmacol Ther 1999; 66: 118–27
Edgar B, Bailey D, Bergstrand R, et al. Acute effects of drinking grapefruit juice on the pharmacokinetics and dynamics of felodipine and its potential clinical relevance. Eur J Clin Pharmacol 1992; 42: 313–7
Munoz CE, Ito S, Bend JR, et al. Propafenone interaction with CYP3A4 inhibitors in man [abstract]. Clin Pharmacol Ther 1997; 61: 154
Uno T, Ohkubo T, Sugawara K, et al. Effects of grapefruit juice on the stereoselective disposition of nicardipine in humans: evidence for dominant presystemic elimination at the gut site. Eur J Clin Pharmacol 2000; 56: 643–9
Veronese ML, Gillen LP, Burke JP, et al. Exposure-dependent inhibition of intestinal and hepatic CYP3A4 in vivo by grapefruit juice. J Clin Pharmacol 2003; 43: 831–9
Fuhr U, Muller Peltzer H, Kern R, et al. Effects of grapefruit juice and smoking on verapamil concentrations in steady state. Eur J Clin Pharmacol 2002; 58: 45–53
Kanazawa S, Ohkubo T, Sugawara K. The effects of grapefruit juice on the pharmacokinetics of erythromycin. Eur J Clin Pharmacol 2001; 56: 799–803
Desta Z, Kivisto KT, Lilja JJ, et al. Stereoselective pharmacokinetics of cisapride in healthy volunteers and the effect of repeated administration of grapefruit juice. Br J Clin Pharmacol 2001; 52: 399–407
Weber A, Jager R, Borner A, et al. Can grapefruit juice influence ethinylestradiol bioavailability? Contraception 1996; 53: 41–7
Sigusch H, Hippius M, Henschel L, et al. Influence of grapefruit juice on the pharmacokinetics of a slow release nifedipine formulation. Pharmazie 1994; 49: 522–4
Lilja JJ, Kivisto KT, Backman JT, et al. Effect of grapefruit juice dose on grapefruit juice-triazolam interaction: repeated consumption prolongs triazolam half-life. Eur J Clin Pharmacol 2000; 56: 411–5
Hollander AA, van Rooij J, Lentjes GW, et al. The effect of grapefruit juice on cyclosporine and prednisone metabolism in transplant patients [abstract]. Clin Pharmacol Ther 1995; 57: 318–24
Libersa CC, Brique SA, Motte KB, et al. Dramatic inhibition of miodarone metabolism induced by grapefruit juice. Br J Clin Pharmacol 2000; 49: 373–8
Garg SK, Kumar N, Bhargava VK, et al. Effect of grapefruit juice on carbamazepine bioavailability in patients with epilepsy. Clin Pharmacol Ther 1998; 64: 286–8
Ozdemir M, Aktan Y, Boydag BS, et al. Interaction between grapefruit juice and diazepam in humans. Eur J Drug Metab Pharmacokinet 1998; 23: 55–9
Castro N, Jung H, Medina R, et al. Interaction between grapefruit juice and praziquantel in humans. Antimicrob Agents Chemother 2002; 46: 1614–6
Varis T, Kivisto KT, Neuvonen PJ. Grapefruit juice can increase the plasma concentrations of oral methylprednisolone. Eur J Clin Pharmacol 2000; 56: 489–93
Fuhr U, Klittich K, Staib AH. Inhibitory effect of grapefruit juice and its bitter principal, naringenin, on CYP1A2 dependent metabolism of caffeine in man. Br J Clin Pharmacol 1993; 35: 431–6
van Agtmael MA, Gupta V, van der Graaf CA, et al. The effect of grapefruit juice on the time-dependent decline of artemether plasma levels in healthy subjects. Clin Pharmacol Ther 1999; 66: 408–14
Lee AJ, Chan WK, Harralson AF, et al. The effects of grapefruit juice on sertraline metabolism: an in vitro and in vivo study. Clin Ther 1999; 21: 1890–9
Ho PC, Chalcroft SC, Coville PF, et al. Grapefruit juice has no effect on quinine pharmacokinetics. Eur J Clin Pharmacol 1999; 55: 393–8
Josefsson M, Zackrisson AL, Ahlner J. Effect of grapefruit juice on the pharmacokinetics of amlodipine in healthy volunteers. Eur J Clin Pharmacol 1996; 51: 189–93
Vincent J, Harris SI, Foulds G, et al. Lack of effect of grapefruit juice on the pharmacokinetics and pharmacodynamics of amlodipine. Br J Clin Pharmacol 2000; 50: 455–63
Yasui N, Kondo T, Furukori H, et al. Effects of repeated ingestion of grapefruit juice on the single and multiple oral-dose pharmacokinetics and pharmacodynamics of alprazolam. Psychopharmacology (Berl) 2000; 150: 185–90
Min DI, Ku YM, Geraets DR, et al. Effect of grapefruit juice on the pharmacokinetics and pharmacodynamics of quinidine in healthy volunteers. J Clin Pharmacol 1996; 36: 469–76
Penzak SR, Acosta EP, Turner M, et al. Effect of Seville orange juice and grapefruit juice on indinavir pharmacokinetics. J Clin Pharmacol 2002; 42: 1165–70
Shelton MJ, Wynn HE, Hewitt RG, et al. Effects of grapefruit juice on pharmacokinetic exposure to indinavir in HIV-positive subjects. J Clin Pharmacol 2001; 41: 435–42
Cheng KL, Nafziger AN, Peloquin CA, et al. Effect of grapefruit juice on clarithromycin pharmacokinetics. Antimicrob Agents Chemother 1998; 42: 927–9
Vandel P, Regina W, Reix I, et al. Grapefruit juice as a contraindication? An approach in psychiatry [in French]. Encephale 1999; 25: 67–71
Yasui N, Kondo T, Suzuki A, et al. Lack of significant pharmacokinetic interaction between haloperidol and grapefruit juice. Int Clin Psychopharmacol 1999; 14: 113–8
Tassaneeyakul W, Vannaprasaht S, Yamazoe Y. Formation of omeprazole sulphone but not 5-hydroxyomeprazole is inhibited by grapefruit juice. Br J Clin Pharmacol 2000; 49: 139–44
Christensen H, Asberg A, Holmboe AB, et al. Coadministration of grapefruit juice increases systemic exposure of diltiazem in healthy volunteers. Eur J Clin Pharmacol 2002; 58: 515–20
Sigusch H, Henschel L, Kraul H, et al. Lack of effect of grapefruit juice on diltiazem bioavailability in normal subjects. Pharmazie 1994; 49: 675–9
Jetter A, Kinzig Schippers M, Walchner Bonjean M, et al. Effects of grapefruit juice on the pharmacokinetics of sildenafil. Clin Pharmacol Ther 2002; 71: 21–9
Zaidenstein R, Soback S, Gips M, et al. Effect of grapefruit juice on the pharmacokinetics of losartan and its active metabolite E3174 in healthy volunteers. Ther Drug Monit 2001; 23: 369–73
Lane HY, Jann MW, Chang YC, et al. Repeated ingestion of grapefruit juice does not alter clozapine’s steady-state plasma levels, effectiveness, and tolerability. J Clin Psychiatry 2001; 62: 812–7
Vandel S, Netillard C, Perault MC, et al. Plasma levels of clozapine and desmethylclozapine are unaffected by concomitant ingestion of grapefruit juice. Eur J Clin Pharmacol 2000; 56: 347–8
van Rooij J, van der Meer FJM, Schoemaker HC, et al. Comparison of the effect of grapefruit juice and cimetidine on pharmacokinetics and anticoagulant effect of a single dose of acenocoumarol [abstract]. Br J Clin Pharmacol 1993; 35: 548
Kumar N, Garg SK, Prabhakar S. Lack of pharmacokinetic interaction between grapefruit juice and phenytoin in healthy male volunteers and epileptic patients. Methods Find Exp Clin Pharmacol 1999; 21: 629–32
Fukazawa I, Uchida N, Uchida E, et al. Effects of grapefruit juice on pharmacokinetics of atorvastatin and pravastatin in Japanese. Br J Clin Pharmacol 2004; 57: 448–55
Banfield C, Gupta S, Marino M, et al. Grapefruit juice reduces the oral bioavailability of fexofenadine but not desloratadine. Clin Pharmacokinet 2002; 41: 311–8
Penzak SR, Gubbins PO, Gurley BJ, et al. Grapefruit juice decreases the systemic availability of itraconazole capsules in healthy volunteers. Ther Drug Monit 1999; 21: 304–9
Demarles D, Gillotin C, Bonaventure Paci S, et al. Single-dose pharmacokinetics of amprenavir coadministered with grapefruit juice. Antimicrob Agents Chemother 2002; 46: 1589–90
Reif S, Nicolson MC, Bisset D, et al. Effect of grapefruit juice intake on etoposide bioavailability. Eur J Clin Pharmacol 2002; 58: 491–4
Gupta MC, Garg SK, Badyal D, et al. Effect of grapefruit juice on the pharmacokinetics of theophylline in healthy male volunteers. Methods Find Exp Clin Pharmacol 1999; 21: 679–82
Mayol RF, Adamson DS, Gammans RE, et al. Pharmacokinetics and disposition of 14C-buspirone HC1 after intravenous and oral dosing in man [abstract]. Clin Pharmacol Ther 1985; 37: 210
Kivisto KT, Lamberg TS, Neuvonen PJ. Interactions of buspirone with itraconazole and rifampicin: effects on the pharmacokinetics of the active 1-(2-pyrimidinyl)-piperazine metabolite of buspirone. Pharmacol Toxicol 1999; 84: 94–7
Bailey DG. Grapefruit juice-drug interaction issues. In: Boullata J, Armeni V, editors. Handbook of drug-nutrient interactions. Totawa (NJ): The Humana Press, 2004: 175–194
Rogers JD, Zhao J, Liu L, et al. Grapefruit juice has minimal effects on plasma concentrations of lovastatin-derived 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors. Clin Pharmacol Ther 1999; 66: 358–66
Willner K. Excretion and decomposition of 3-methoxy-N-methylmorphinan and its demethylated derivatives in man [in German]. Arzneimittel Forschung 1963; 13: 26–9
Talajic M, DeRoode MR, Nattel S. Comparative electrophysiologic effects of intravenous amiodarone and desethylamiodarone in dogs: evidence for clinically relevant activity of the metabolite. Circulation 1987; 75: 265–71
Zhou L, Chen BP, Kluger J, et al. Effects of amiodarone and its active metabolite desethylamiodarone on the ventricular defibrillation threshold. J Am Coll Cardiol 1998; 31: 1672–8
Ku YM, Min DI, Flanigan M. Effect of grapefruit juice on the pharmacokinetics of microemulsion cyclosporine and its metabolite in healthy volunteers: does the formulation difference matter? J Clin Pharmacol 1998; 38: 959–65
Brunner LJ, Pai KS, Munar MY, et al. Effect of grapefruit juice on cyclosporin A pharmacokinetics in pediatric renal transplant patients. Pediatr Transplant 2000; 4: 313–21
Hermann M, Asberg A, Reubsaet JL, et al. Intake of grapefruit juice alters the metabolic pattern of cyclosporin A in renal transplant recipients. Int J Clin Pharmacol Ther 2002; 40: 451–6
Venkatakrishnan K, von Moltke LL, Greenblatt DJ. Effects of the antifungal agents on oxidative drug metabolism: clinical relevance. Clin Pharmacokinet 2000; 38: 111–80
Kaukonen KM, Olkkola KT, Neuvonen PJ. Fluconazole but not itraconazole decreases the metabolism of losartan to E-3174. Eur J Clin Pharmacol 1998; 53: 445–9
Lippert C, Ling J, Brown P, et al. Mass balance and pharmacokinetics of MDL 16455A in healthy male volunteers [abstract]. Pharm Res 1995; 12: S390
Gubbins PO, McConnell SA, Gurley BJ, et al. Influence of grapefruit juice on the systemic availability of itraconazole oral solution in healthy adult volunteers. Pharmacotherapy 2004; 24: 460–7
Dresser GK, Bailey DG, Carruthers SG. Grapefruit juice: felodipine interaction in the elderly. Clin Pharmacol Ther 2000; 68: 28–34
Bailey DG, Dresser GK. Interactions between grapefruit juice and cardiovascular drugs. Am J Cardiovasc Drugs 2004; 4: 281–97
Lilja JJ, Juntti-Patinen L, Neuvonen PJ. Orange juice substantially reduces the bioavailability of the beta-adrenergic-blocking agent celiprolol. Clin Pharmacol Ther 2004; 75: 184–90
Malhotra S, Bailey DG, Paine MF, et al. Seville orange juicefelodipine interaction: comparison with dilute grapefruit juice and involvement of furocoumarins. Clin Pharmacol Ther 2001; 69: 14–23
Backman JT, Maenpaa J, Belle DJ, et al. Lack of correlation between in vitro and in vivo studies on the effects of tangeretin and tangerine juice on midazolam hydroxylation. Clin Pharmacol Ther 2000; 67: 382–90
Silverman JA, Thorgeirsson SS. Regulation and function of the multidrug resistance genes in liver. Prog Liver Dis 1995; 13: 101–23
Cvetkovic M, Leake B, Fromm MF, et al. OATP and P-glycoprotein transporters mediate the cellular uptake and excretion of fexofenadine. Drug Metab Dispos 1999; 27: 866–71
Kim RB. Organic anion-transporting polypeptide (OATP) transporter family and drug disposition. Eur J Clin Invest 2003; 33Suppl. 2: 1–5
Ranganna S, Govindarajan VS, Ramana KV. Citrus fruits: varieties, chemistry, technology, and quality evaluation. Part II: chemistry, technology, and quality evaluation. A. Chemistry. Crit Rev Food Sci Nutr 1983; 18: 313–86
Bailey DG, Arnold JM, Spence JD. Grapefruit juice and drugs: how significant is the interaction? Clin Pharmacokinet 1994: 26: 91–8
Kuhnau J. The flavonoids: a class of semi-essential food components: their role in human nutrition. World Rev Nutr Diet 1976; 24: 117–91
Cheng KJ, Krishnamurty HG, Jones GA, et al. Identification of products produced by the anaerobic degradation of naringin by Butyrivibrio sp. C3. Can J Microbiol 1971; 17: 129–31
Fuhr U, Kummert AL. The fate of naringin in humans: a key to grapefruit juice-drug interactions? Clin Pharmacol Ther 1995; 58: 365–73
Bailey DG, Arnold JM, Munoz C, et al. Grapefruit juice: felodipine interaction. Mechanism, predictability, and effect of naringin. Clin Pharmacol Ther 1993; 53: 637–42
Bailey DG, Arnold JM, Strong HA, et al. Effect of grapefruit juice and naringin on nisoldipine pharmacokinetics. Clin Pharmacol Ther 1993; 54: 589–94
Bailey DG, Munoz C, Arnold JMO, et al. Grapefruit juice and naringin interaction with nitrendipine [abstract]. Clin Pharmacol Ther 1992; 51: 156
Bailey DG, Kreeft JH, Munoz C, et al. Grapefruit juice-felodipine interaction: effect of naringin and 6′,7′-dihydroxybergamottin in humans. Clin Pharmacol Ther 1998; 64: 248–56
Kakar SM, Paine MF, Stewart PW, et al. 6′7′-Dihydroxybergamottin contributes to the grapefruit juice effect. Clin Pharmacol Ther 2004; 75: 569–79
Ohnishi A, Matsuo H, Yamada S, et al. Effect of furanocoumarin derivatives in grapefruit juice on the uptake of vinblastine by Caco-2 cells and on the activity of cytochrome P450 3A4. Br J Pharmacol 2000; 130: 1369–77
Tassaneeyakul W, Guo LQ, Fukuda K, et al. Inhibition selectivity of grapefruit juice components on human cytochromes P450. Arch Biochem Biophys 2000; 378: 356–63
Eagling VA, Profit L, Back DJ. Inhibition of the CYP3A4-mediated metabolism and P-glycoprotein-mediated transport of the HIV-1 protease inhibitor saquinavir by grapefruit juice components. Br J Clin Pharmacol 1999; 48: 543–52
Ikegawa T, Ushigome F, Koyabu N, et al. Inhibition of P-glycoprotein by orange juice components, polymethoxyflavones in adriamycin-resistant human myelogenous leukemia (K562/ADM) cells. Cancer Lett 2000; 160: 21–8
Takanaga H, Ohnishi A, Yamada S, et al. Polymethoxylated flavones in orange juice are inhibitors of P-glycoprotein but not cytochrome P450 3A4. J Pharmacol Exp Ther 2000; 293: 230–6
Manthey JA, Grohmann K. Phenols in citrus peel byproducts: concentrations of hydroxycinnamates and polymethoxylated flavones in citrus peel molasses. J Agric Food Chem 2001; 49: 3268–73
Acknowledgements
This work was supported by a grant from the Ministry of Health, Labour and Welfare, Japan. The authors have no conflicts of interest directly relevant to the content of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Saito, M., Hirata-Koizumi, M., Matsumoto, M. et al. Undesirable Effects of Citrus Juice on the Pharmacokinetics of Drugs. Drug-Safety 28, 677–694 (2005). https://doi.org/10.2165/00002018-200528080-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002018-200528080-00003