
Abstract
Background and objectives: Gefitinib (IRESSA®, ZD1839), an epidermal growth factor receptor tyrosine kinase inhibitor, has been approved in several countries for the treatment of advanced non-small-cell lung cancer. Preclinical studies were conducted to determine the cytochrome P450 (CYP) isoenzymes involved in the metabolism of gefitinib and to evaluate the potential of gefitinib to cause drug interactions through inhibition of CYP isoenzymes. Based on these findings, three clinical studies were carried out to investigate pharmacokinetic drug interactions in vivo with gefitinib.
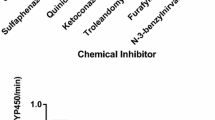
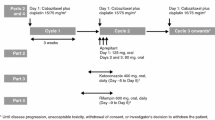
Methods: In preclinical studies radiolabelled gefitinib was incubated with: (i) hepatic microsomal protein in the presence of selective CYP inhibitors; and (ii) expressed CYP enzymes. Human hepatic microsomal protein was incubated with selective CYP substrates in the presence of gefitinib. Clinical studies were all phase I, open-label, single-centre studies; two had a randomised, two-way crossover design and the third was nonrandomised. The first and second studies investigated the pharmacokinetics of gefitinib in the presence of a potent CYP3A4 inducer (rifampicin [rifampin]) or inhibitor (itraconazole) in healthy male volunteers. The third study investigated the effects that gefitinib had on the pharmacokinetics of metoprolol, a CYP2D6 substrate, in patients with solid tumours.
Results: The results of preclinical studies demonstrated that CYP3A4 is involved in the metabolism of gefitinib and that gefitinib is a weak inhibitor of CYP2D6 activity. In clinical studies when gefitinib was administered in the presence of rifampicin, geometric mean (gmean) maximum concentration and area under the plasma concentration-time curve (AUC) were reduced by 65% and 83%, respectively; these changes were statistically significant. When gefitinib was administered in the presence of itraconazole, gmean AUC increased by 78% and 61% at gefitinib doses of 250 and 500mg, respectively; these changes also being statistically significant. Coadministration of metoprolol with gefitinib resulted in a 35% increase in the metoprolol area under plasma concentration-time curve from time zero to the time of the last quantifiable concentration; this change was not statistically significant. There was no apparent change in the safety profile of gefitinib as a result of coadministration with other agents.
Conclusions: Although CYP3A4 inducers may reduce exposure to gefitinib, further work is required to define any resultant effect on the efficacy of gefitinib. Exposure to gefitinib is increased by coadministration with CYP3A4 inhibitors, but since gefitinib is known to have a good tolerability profile, a dosage reduction is not recommended. Gefitinib is unlikely to exert a clinically relevant effect on the pharmacokinetics of drugs that are dependent on CYP2D6-mediated metabolism for their clearance, but the potential to increase plasma concentrations should be considered if gefitinib is coadministered with CYP2D6 substrates that have a narrow therapeutic index or are individually dose titrated.













Similar content being viewed by others

Notes
The use of trade names is for product identification purposes only and does not imply endorsement.
References
Traxler P. Tyrosine kinases as targets in cancer therapies: successes and failures. Expert Opin Ther Targets 2003; 7: 215–34
Mendelsohn J, Baselga J. The EGF receptor family as targets for cancer therapy. Oncogene 2000; 19: 6550–65
Wakeling AE, Barker AJ, Davies DH, et al. Specific inhibition of epidermal growth factor receptor tyrosine kinase by 4-anilinoquinazolines. Breast Cancer Res Treat 1996; 38: 67–73
Hammond LA. Pharmacokinetic evaluation of gefitinib when administered with chemotherapy. Clin Lung Cancer 2003; 5 Suppl. 1: S18–21
Bertz RJ, Granneman GR. Use of in vitro and in vivo data to estimate the likelihood of metabolic pharmacokinetic interactions. Clin Pharmacokinet 1997; 32: 210–58
Rodrigues AD. Use of in vitro human metabolism studies in drug development. Biochem Pharmacol 1994; 48: 2147–56
McKillop D, Wild MJ, Butters CJ, et al. Effects of propofol on human hepatic microsomal cytochrome P450 activities. Xenobiotica 1998; 28: 845–53
Jones HK, Stafford LE, Swaisland HC, et al. A sensitive assay for ZD1839 (Iressa) in human plasma by liquid-liquid extraction and high performance liquid chromatography with mass spectrometric detection: validation and use in phase I clinical trials. J Pharm Biomed Anal 2002; 29: 221–8
Swart KJ, Papgis M. Automated high-performance liquid chromatographic method for the determination of rifampicin in plasma. J Chromatog A 1992; 593: 21–4
Cooper KJ, Martin PD, Dane AL, et al. Effect of itraconazole on the pharmacokinetics of rosuvastatin. Clin Pharmacol Ther 2003; 73: 322–9
Rau T, Heide R, Bergmann K, et al. Effect of CYP2D6 genotype on metoprolol metabolism persists during long-term treatment. Pharmacogenetics 2002; 12: 465–72
Ranson M, Hammond LA, Ferry D, et al. ZD1839, a selective oral epidermal growth factor receptor-tyrosine kinase inhibitor, is well tolerated and active in patients with solid, malignant tumors: results of a phase I trial. J Clin Oncol 2002; 20: 2240–50
Ohnhaus EE, Breckenridge AM, Park BK. Urinary excretion of 6β-hydroxycortisol and the time course measurement of enzyme induction in man. Eur J Clin Pharmacol 1989; 36: 39–46
Park BK, Ohnhaus EE. Urinary 6β-hydroxycortisol: a simple, non-invasive index of enzyme induction in man. Das Artzliche Laboratorium 1983; 29: 53–8
Williamson KM, Patterson JH, McQueen RH, et al. Effects of erythromycin or rifampicin on losartan pharmacokinetics in healthy volunteers. Clin Pharmacol Ther 1998; 63: 316–23
Data on file, AstraZeneca, 2002
Venkatakrishnan K, von Moltke LL, Greenblatt DJ. Effects of the antifungal agents on oxidative drug metabolism: clinical relevance. Clin Pharmacokinet 2000; 38: 111–80
Haria M, Bryson HM, Goa KL. Itraconazole: a reappraisal of its pharmacological properties and therapeutic use in the management of superficial fungal infections. Drugs 1996; 51: 585–620
Varhe A, Olkkola KT, Neuvonen PJ. Oral triazolam is potentially hazardous to patients receiving systemic antimycotics ketoconazole or itraconazole. Clin Pharmacol Ther 1994; 56: 601–7
Kivisto KT, Lamberg TS, Kantola T, et al. Plasma buspirone concentrations are greatly increased by erythromycin and itraconazole. Clin Pharmacol Ther 1997; 62: 348–54
Kaukonen KM, Olkkola KT, Neuvonen PJ. Itraconazole increases plasma concentrations of quinidine. Clin Pharmacol Ther 1997; 62: 510–7
Backman JT, Kivisto KT, Olkkola KT, et al. The area under the plasma concentration-time curve for oral midazolam is 400fold larger during treatment with itraconazole than with rifampicin. Eur J Clin Pharmacol 1998; 54: 53–8
Hardman JG, Limbird LE, Gilman AG, editors. Goodman and Gilman’s the pharmacological basis of therapeutics. 10th ed. New York: McGraw-Hill, 2001: 255–6
Acknowledgements
The authors would like to acknowledge the analytical and technical support provided by Analytico Medinet, The Netherlands; Pharma Bio-Research, The Netherlands; and BAS Analytics, UK, as well as in-house support from the Drug Metabolism and Pharmacokinetics Department of AstraZeneca, for analysis of the plasma samples. We thank the research staff at the investigator sites and within the Experimental Medicines Department of AstraZeneca for their participation in the conduct of the studies.
Funding for this study was provided by AstraZeneca. The authors have no conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Swaisland, H.C., Ranson, M., Smith, R.P. et al. Pharmacokinetic Drug Interactions of Gefitinib with Rifampicin, Itraconazole and Metoprolol. Clin Pharmacokinet 44, 1067–1081 (2005). https://doi.org/10.2165/00003088-200544100-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-200544100-00005