


Abstract
Siberian ginseng ([SG]; Eleutherococcus senticosus) is a commonly used herbal preparation. The objective of this study was to assess in normal volunteers (n = 12) the influence of a standardized SG extract on the activity of cytochrome P450 CYP2D6 and 3A4. Probe substrates dextromethorphan (CYP2D6 activity) and alprazolam (CYP3A4 activity) were administered orally at baseline and again following treatment with SG (1 × 485 mg twice daily) for 14 days. Urinary concentrations of dextromethorphan and dextorphan were quantified, and dextromethorphan metabolic ratios (DMRs) were determined at baseline and after SG treatment. Likewise, plasma samples were collected (0–60 h) for alprazolam pharmacokinetics at baseline and after SG treatment to assess effects on CYP3A4 activity. Validated high performance liquid chromatography methods were used to quantify all compounds and relevant metabolites. There were no statistically significant differences between pre- and post-SG treatment DMRs indicating a lack of effect on CYP2D6 (P > 0.05). For alprazolam there also were no significant differences in the pharmacokinetic parameters determined by noncompartmental modeling (Cmax, Tmax, area under the curve, half-life of elimination) indicating that SG does not significantly induce or inhibit CYP3A4 (P > 0.05). Our results indicate that standardized extracts of SG at generally recommended doses for over-the-counter use are unlikely to alter the disposition of coadministered medications primarily dependent on the CYP2D6 or CYP3A4 pathways for elimination.
There has been a dramatic increase in the use of herbal dietary supplements in the United States and Europe (Brevoort, 1998; Eisenberg et al., 1998). SG1 is among the 10 most popular supplements used in the United States (Li, 2001). It is derived from the roots of Eleutheroccus senticosus and is purported to behave as an “adaptogen”, a class of herbal medications that confer resistance to the effects of stress (Gaffney et al., 2001). Although SG has been used in Chinese medicine for over 4000 years, it should not be confused with “True” or “Asian ginseng”, which is derived fromPanax ginseng, another genus and species in the Araliaceae family. SG is more commonly used in the United States (Li, 2001).
SG contains a unique array of biologically active constituents. The eleutherosides (Fig. 1) have been given the most attention and are believed responsible for the proposed adaptogenic activity. Most commercially available extracts have been standardized according to the content of eleutheroside B (syringin 4-β-d-glucoside) and eleutheroside E (syringaresinol 4, 4′ β-d-diglucoside). Other components with reported biological activities include sesamin, β-sitosterol, hedarasaponin B, and isofraxidin as well as various flavonoids and hydroxycinnamates (Davydov and Krikorian, 2000).

Structures of eleutheroside B and eleutheroside E from SG (Eleutherococcus senticosus).
Glucose moieties on both molecules are connected by β-glycosidic linkages.
The Dietary Supplement Health and Education Act of 1994 permits the direct marketing of SG as well as other herbal products and supplements to consumers in the United States without Food and Drug Administration regulation. Thus, there is no current requirement to demonstrate their safety and efficacy. However, the need for further research in the area is underscored by reports of clinically significant drug interactions with Saint John's Wort (Ernst, 2000; Markowitz and DeVane, 2001). No previous clinical studies have assessed the potential for SG to participate in drug interactions. One study reported that whole extracts of SG did not inhibit the activity of human CYP3A4 activity using isolated cDNA-expressed human liver microsomes (Budzinski et al., 2000).
The present study assessed the drug interaction potential of SG in normal volunteers. We specifically sought to assess the effect of SG on the activity of CYP3A4 and CYP2D6, two predominant isoforms (Brosen, 1996). Dextromethorphan (DM) was chosen as a probe drug for CYP2D6 due to its known tolerability, safety, validity as a CYP2D6 phenotypic probe, and extensive use in drug interaction studies (Smith et al., 1998). Alprazolam (ALPZ) was chosen as a probe compound for CYP3A4 activity since it is a relatively pure substrate for CYP3A4 isoforms (Venkatakrishnan et al., 1998; Gorski et al., 1999; Schmider et al., 1999). It has been used effectively as a probe of CYP3A4 activity in a number of published studies (Furukori et al., 1998; Schmider et al., 1999).
Materials and Methods
Subjects.
Twelve volunteers (7 male, 5 female) ages 23 to 44 yrs (33.3 ± 10.2 years; 74.5 ± 14.4 kg) provided informed consent approved by the Medical University of South Carolina's Office of Research Integrity. All were determined to be healthy by history, physical exam, basic laboratory indices, and ECG. Subjects were nonsmokers, taking no medications, and abstained from caffeine, ethanol, and grapefruit juice during the study. All were phenotyped as normal metabolizers of CYP2D6 (Schmid et al., 1985).
Study Design and Drug Administration.
Subjects were admitted to the Medical University of South Carolina General Clinical Research Center. Following an overnight fast and urinary void, each subject was given 30 mg DM (Robitussin Maximum Strength Cough syrup, Madison, NJ) and 2 mg ALPZ (Mylan Pharmaceuticals, Morgantown, WV) orally with 30 to 60 ml of water. Subjects were fed a standard breakfast 30 to 45 min following drug administration. An 8-h urine collection commenced immediately after drug administration. Blood samples were obtained in heparinized tubes prior (i.e., 0 h) to drug administration, and again at 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12, 24, 36, 48, and 60-h time points. This phase served as the baseline measurement of CYP2D6 and CYP3A4 activity.
After a minimum 7-day wash-out period, subjects were provided a 14-day supply of the standardized SG extract (Nature's Way, Springville, UT) with instructions to take one 485-mg capsule twice daily at 8:00 AM and 8:00 PM. SG capsules were dispensed in “medication minders”, in an effort to enhance subject compliance with dosing and aid in tablet counting (Park et al., 1991).
After 14 days of treatment with SG, subjects were re-admitted to the General Clinical Research Center and dosed with 30 mg DM and 2 mg ALPZ as in the baseline phase with identical specimen collection times and identical meals. Additionally, one SG capsule was given concomitantly with the ALPZ and DM and continued at 8:00 AM and 8:00 PM for one day thereafter.
Analytical Methods.
The content of the main active ingredients in SG were analyzed to confirm that levels were in agreement with labeled claims. The formulation used in this study reportedly contained 250 mg of a concentrated SG extract standardized to 0.3% eleutheroside B and 0.5% eleutheroside E mixed with 235 mg ground SG root (total capsule weight = 485 mg). Three replicate analyses of eleutheroside B and E were performed on five combined capsules from the lot used in the present study. The powder from the capsules was further pulverized, dissolved in methanol (1 mg/ml), and analyzed using HPLC with detection at 215 nm (Luna C18 (2) 250 × 4.6 mm, 5 μm column; Phenomonex, Torrance, CA; gradient elution from 10 to 30% acetonitrile in aqueous 0.5% H3P04 over 40 min). Compounds were identified by their retention times in comparison with analytical standards (Chromadex, Laguna Hills, CA).
DM and dextorphan and ALPZ were determined using a previously described HPLC methods (Miller and DeVane, 1988; Hoskins et al., 1997). The pharmacokinetic program WinNonlin (Pharsight, Mountain View, CA) was used to estimate pharmacokinetic parameters. Mean pharmacokinetic parameters and DMRs at baseline and following SG administration were analyzed using the paired t test. Data were also sorted by sex and analyzed using the same methodology as sex-specific induction of CYP3A4 has been reported (Gurley et al., 2002). The level of significance was set at p = 0.05.
Results and Discussion
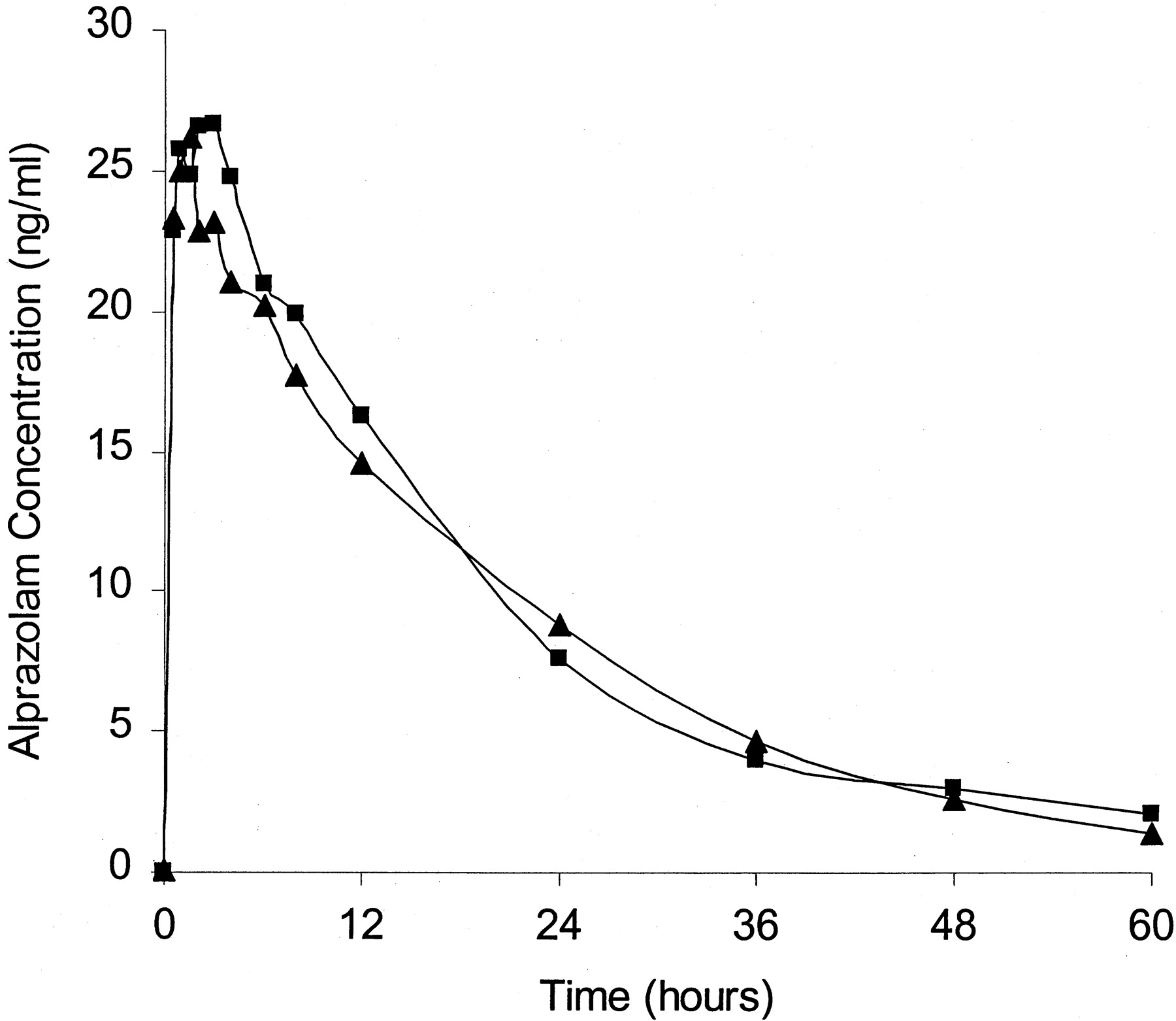
All twelve subjects completed the study, and nausea in one subject after SG administration was the only reported adverse event. CYP2D6 activity was assessed by the ratio of DM to its metabolite. All subjects metabolized DM extensively at baseline and after SG administration. In four individuals only the metabolite was present in detectable quantities during at least one of the phases, and the ratio was considered to be 0.000. The ratio of DM to its metabolite was 0.003 + 0.004 at baseline and 0.005 + 0.008 after SG. There were no significant differences in the ratios between the baseline and SG phases (P > 0.05). CYP3A4 activity was assessed by analysis of ALPZ pharmacokinetics. The observed mean concentration versus time curves from 0 to 60 h for all volunteers at baseline and following SG are shown in Fig.2, and pharmacokinetic parameters are summarized in Table 1. None of the values were significantly different between treatment phases (P > 0.05). When data were sorted by sex, and analyzed separately for each group using, none of the pharmacokinetic values emerged as statistically significant.

Mean plasma alprazolam concentration versus time profile for all subjects (n = 12) following administration of 2 mg alprazolam before (▪) and after (▴) treatment with SG, two 485-mg tablets twice daily for 14 days.
Pharmacokinetic parameters of alprazolam at baseline and after Siberian ginseng administration
These results indicate that standardized extracts of SG are unlikely to alter the disposition of coadministered medications primarily dependent on the CYP2D6 or CYP3A4 pathways for metabolism. This conclusion is based on the finding that there were no significant differences in the DMR or any of the major pharmacokinetic parameters of ALPZ. Furthermore, the mean values for ALPZ clearance were nearly identical after both phases indicating that steady-state concentrations of CYP3A4 substrates would be unaffected by coadministration of SG.
This study is not without its limitations. We cannot preclude the possibility of simultaneous inhibition and induction of CYP3A4 by one or more constituents of the SG. We also did not study the effect of SG on other important isoforms of P450 such as 1A2, 2C9, or 2C19 or the effect on Phase II enzymes or drug transporters. A recent report describes a patient with elevated digoxin levels while taking SG (McRae, 1996). An explanation for this apparent drug interaction would be the ability of SG to inhibit MDR-1 (P-glycoprotein), (Hoffemeyer et al., 2000). Our study did not assess the ability of SG to inhibit MDR-1 as ALPZ is apparently not a substrate for this transporter (Greenblatt, personal communication).
In this study, unlike most previous studies, the SG extract has been characterized with respect to the content of the major biologically active ingredients, eleutherosides B and E, which can deviate substantially from the labeled content (Harkey et al., 2001; Kressman et al., 2002). A chromatogram of the SG extract used in the present study is shown in Fig. 3. Each capsule contained 2.1 ± 0.3 mg of eleutheroside B and 4.1 + 0.2 mg of eleutheroside E, levels that are 40 to 50% higher than reported by the manufacturer. We used a formulation containing both a concentrated extract and the ground root, both of which certainly contain other components in addition to the eleutherosides. Our results indicate that components of both the root and extract fail to produce any change in P450 activity.

High performance liquid chromatogram of the Siberian ginseng extract used in this study.
The extract was standardized to the main active components eleutheroside B (B) and eleutheroside E (E).
In conclusion, the results suggest that standardized SG extracts, when taken in normally recommended doses, do not affect the activity of CYP2D6 or CYP3A4. There appears to be little likelihood of significant botanical-drug interactions between SG and drugs predominantly metabolized by CYP2D6 or CYP3A4 isoforms.
Footnotes
-
This study was sponsored by Public Health Service Grant NCCAM R21 AT00511−01.
- Abbreviations used are::
- SG
- Siberian ginseng
- DM
- dextromethorphan
- ALPZ
- alprazolam
- DMR
- dextromethorphan metabolic ratio
- Received December 10, 2002.
- Accepted January 17, 2003.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}