


Abstract
Prohormones such as 19-norandrostenediol (estr-4-ene-3β,17β-diol) have been added to the list of prohibited substances of the World Anti-Doping Agency because they are metabolized to the common nandrolone metabolites norandrosterone and noretiocholanolone. So far, no studies on the metabolism and in vivo conversion of 19-norandrostenediol after oral or sublingual administration have been reported nor have had quantified data on resulting plasma nandrolone levels. In the present study, an open-label crossover trial with eight healthy male volunteers was conducted. After application of capsules or sublingual tablets of 19-norandrostenediol plasma concentrations of 19-norandrostenediol, nandrolone as well as major metabolites (19-norandrosterone and 19-noretiocholanolone) were determined using a validated assay based on gas chromatography/mass spectrometry. The administration of 100-mg capsules of 19-norandrostenediol yielded maximum plasma total concentrations (i.e., conjugated plus unconjugated compounds) of 1.1 ng/ml (±0.7) for 19-norandrostenediol, 4.0 ng/ml (±2.6) for nandrolone, 154.8 ng/ml (±130.8) for 19-norandrosterone, and 37.7 ng/ml (±6.9) for 19-noretiocholanolone. The use of 25-mg sublingual tablets resulted in 3.3 ng/ml (±1.0) for 19-norandrostenediol, 11.0 ng/ml (±6.4) for nandrolone, 106.3 ng/ml (±40.1) for 19-norandrosterone, and 28.5 ng/ml (±20.8) for 19-noretiocholanolone. Most interestingly, the pharmacologically active unconjugated nandrolone was determined after administration of sublingual tablets (up to 5.7 ng/ml) in contrast to capsule applications. These results demonstrate the importance of prohibiting prohormones such as 19-norandrostenediol, in particular, since plasma concentrations of nandrolone between 0.3 to 1.2 ng/ml have been reported to influence endocrinological parameters.
Nandrolone (NL; Fig. 1A) is an anabolic steroid usually administered as the decanoate ester in the form of oily intramuscular injections. Nandrolone has been used as an anabolic agent after debilitating illness and for the treatment of postmenopausal osteoporosis, post-menopausal metastatic breast carcinoma, anemia as a result of chronic renal failure, and aplastic anemia. In addition to these therapeutic applications, NL gained public recognition because of its abuse by athletes for the purpose of increasing muscle mass and muscular strength (Yesalis and Bahrke, 1995). As a result, NL, among others, was banned in 1974 by the International Olympic Committee. To provide evidence of NL doping, the main urinary metabolites 19-norandrosterone (NA; Fig. 1B) and 19-noretiocholanolone (NE; Fig. 1C) have been used as target analytes (Schänzer and Donike, 1993; Schänzer, 1996; Saugy et al., 2000; Kicman and Gower, 2003). As a reference, NA has to exceed a threshold level of 2 ng per ml of urine to produce a positive doping test result. In its 2004 Adverse Analytical Findings Reported by Accredited Laboratories (http://www.wadaama.org/rtecontent/document/LABSTATS_2004.pdf; access date 6-14-2006), the World Anti-Doping Agency (WADA) listed 339 positive specimens related to nandrolone abuse, which represented a proportion of 10% of the overall doping offenses detected in the WADA-accredited laboratories. As recently published, not only deliberate appliance of nandrolone products have led to verifiable concentrations of NA in urine but also the degradation of endogenously produced androsterone to NA in so-called “active” urine specimens (Grosse et al., 2005). Moreover, the administration of contaminated nutritional supplements (Catlin et al., 2000; Geyer et al., 2004) and possible endogenous production of nandrolone (Le Bizec et al., 1999; Kohler and Lambert, 2002) are associated with the detection of NA in urine samples. In particular, the ingestion of nutritional supplements containing 19-norandrostenedione (ND; Fig. 1D) and 19-norandrostenediol (NDiol; Fig. 1E) resulted in positive drug tests, owing to the presence of NA (Uralets and Gillette, 1999; Colker et al., 2001; Tseng et al., 2005). Supplement companies introduced both so-called prohormones as legal alternatives to illegal androgens in 1998, and anabolic properties were advertised because of an assumed conversion to NL. Since 1999, ND and NDiol were classified as anabolic agents as defined by the International Olympic Committee Anti-Doping Code and, as such, were banned in most sports. Under the disguise of The Dietary Supplement Health and Education Act, these prohormones were available as nutritional supplements for over-the-counter sales in the United States until the commencement of the Anabolic Steroid Control Act of 2004. Several studies on nandrolone prohormones dealing with the analysis of urinary metabolites or effects on athletic performance have recently been conducted (Uralets and Gillette, 1999; Colker et al., 2001; Van Gammeren et al., 2001, 2002; Tseng et al., 2005), but with the exception of the results of a pilot study (Machnik et al., 2001), no scientific data were published dealing with the in vivo conversion of these hormone precursors to their active form, i.e., NL. To investigate the in vivo biotransformation of NDiol, an evaluation of plasma levels of 19-norsteroids, in particular, of unconjugated nandrolone (NLunc), was performed within a clinical trial. To gain information on whether the route of administration affects the metabolic rate of the compound, NDiol was tested, formulated as capsules as well as sublingual tablets.
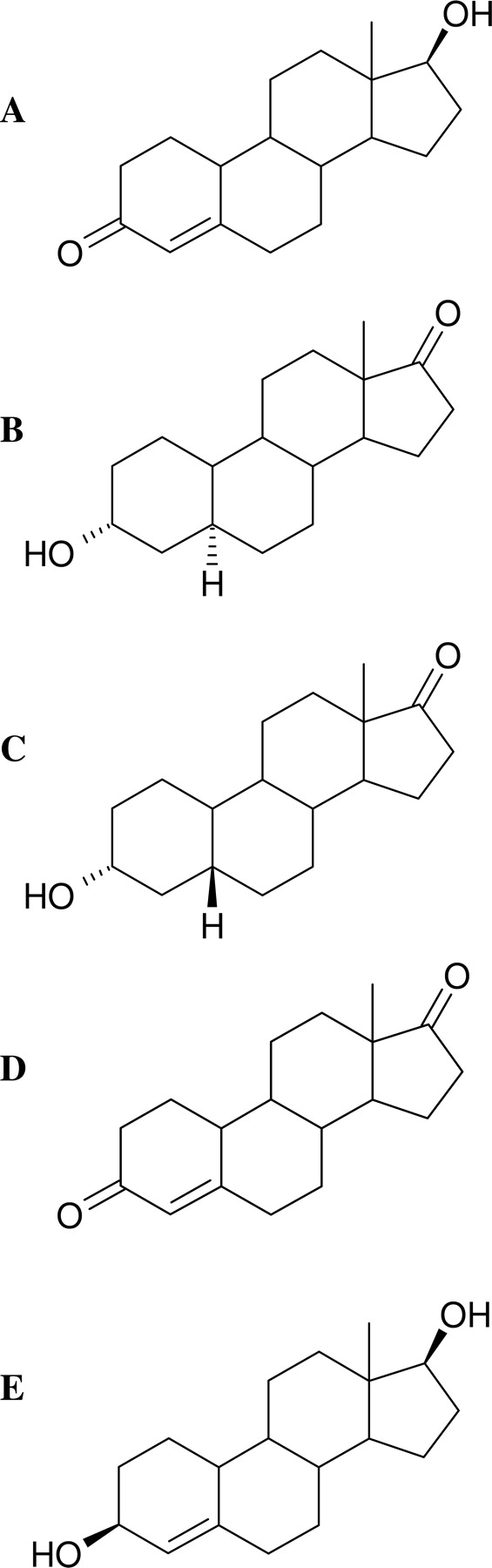
Chemical structures of NL (A; mol. wt., 274), NA (B; mol. wt., 276), NE (C; mol. wt., 276), ND (D; mol. wt., 272), and NDiol (E; mol. wt., 276).
Materials and Methods
Chemicals. Potassium hydroxide (p.a.), sodium hydroxide (p.a.), and sodium dihydrogen phosphate monohydrate (p.a.) were purchased from Merck (Darmstadt, Germany). β-Glucuronidase from Escherichia coli was supplied by Roche Diagnostics (Mannheim, Germany). Methanol and tert-butyl methyl ether were obtained from Kraemer and Martin (St. Augustin, Germany) and distilled before use. n-Pentane (≥99%) was bought from Merck Schuchard (Hohenbrunn, Germany). N-Methyl-N-trimethylsilyltrifluoroacetamide was supplied by Chem. Fabrik Karl Bucher (Waldstetten, Germany) and distilled before use. Ammonium iodide and ethanethiol (≥97%) were purchased from Sigma-Aldrich (Steinheim, Germany).
Steroids. Nandrolone (>99%) was bought from Sigma-Aldrich, and d3-NE (98%) was purchased from LGC Promochem (Wesel, Germany). The steroids NDiol (95%), NA (>97%), NE (>97%), d3-NDiol [3β/3α-isomers 3:1 (w/w)], and d3-NL (96%) were synthesized in our laboratory according to established procedures (Schänzer and Donike, 1993, 1995).
Subjects. Eight healthy men (age, 32.8 ± 7.5 years; weight, 81.6 ± 10.7 kg) volunteered to participate in this study. Before the study, subjects underwent physical examinations to check up on entrance and exclusion criteria (e.g., medical history, physical examinations, hematological tests, and blood and urine evaluations). Each participant read and signed a health history and informed consent that detailed the outline of the study.
Regulatory and Ethical Aspects. According to the German Drugs Act, nutritional supplements containing prohormones such as NDiol have never been considered as food supplements but as drug products without regulatory approval. Because of this status, our present investigation was categorized as a phase I clinical trial. Ethical committee application, study protocol, and informed consent form were prepared in accordance with the Declaration of Helsinki and approved by the Cologne University Human Subjects Committee. Registration at the local health authority and the Federal Institute for Drugs and Medical Advices (Bundesinstitut fur Arzneimittel und Medizinprodukte, Bonn, Germany) was applied.
Supplementation. Two nutritional supplements containing NDiol were purchased via the Internet. Norandrodiol (Kaizen, Los Angeles, CA) was consumed in 100-mg capsules. Cyclo-Nordiol (Kaizen) was provided as sublingual tablets containing a hydroxypropyl-β-cyclodextrin-norandrostenediol complex (25 mg of NDiol per tablet). Supplements were analyzed for purity and authenticity in our laboratory. The study was designed as an open crossover trial. Administration of each of the respective products was performed once for each individual. Supplement administrations were separated by a period of at least 2 weeks. NDiol capsules were swallowed with water. Sublingual NDiol was placed under the tongue and allowed to dissolve for at least 10 min before swallowing tablet residues. Subjects were instructed to fast before and for 2 h after administration of NDiol supplements.
Blood Sample Collection. On the day of administration, an indwelling catheter was inserted into a forearm vein. Blood samples (10 ml) were collected immediately before supplementation and at 10, 20, 30, 45, 60, and 90 min and 2, 3, 4, 6, and 8 h from t = 0. An additional sample was obtained by venipuncture 24 h after administration. Blood samples were collected in potassium-EDTA tubules and centrifuged immediately, and the separated plasma was stored at –20°C until analysis.

Chemical structures of d3-NDiol (A; mol. wt., 279), d3-NL (B; mol. wt., 277), and d3-NE (C; mol. wt., 279).
Plasma Sample Preparation. For each analysis, a volume of 0.5 ml of plasma was used. Each specimen was fortified with 20 μl of an internal standard mixture (0.1 μg/ml d3-NDiol, 0.1 μg/ml d3-NL, and 1.0 μg/ml d3-NE; Fig. 2, A–C).
For the determination of total plasma steroid concentrations (unconjugated plus conjugated steroids; NDioltot, NLtot, NAtot, NEtot), 0.5 ml of phosphate buffer (0.2 M, pH 7) was added, and an enzymatic hydrolysis was performed using 50 μlof β-glucuronidase from E. coli at 50°C for 60 min. After adjusting to pH 12 with 0.5 ml of aqueous KOH (0.5 M), a first liquid-liquid extraction (LLE) was performed by adding 6 ml of tert-butyl methyl ether and shaking for 15 min. After centrifugation for 10 min at 1200g, the organic layer was transferred into a fresh tube and evaporated to dryness. The residue was resuspended in 1.0 ml of sodium hydroxide (0.01 M). A second LLE was carried out using 5 ml of n-pentane and shaking for 15 min. After centrifugation for 10 min at 1200g, the organic phase was collected and re-extracted by shaking with 2 ml of a mixture of methanol/water [95:5 (v/v)] for 15 min. Subsequent centrifugation for 10 min at 1200g was followed by removal of n-pentane and evaporation of the aqueous-methanolic layer. Finally, analytes were derivatized with 50 μl of a mixture of N-methyl-N-trimethylsilyltrifluoroacetamide/NH4I/ethanethiol [1000:2:3 (v/wt/v)] by incubation for 15 min at 60°C. For the determination of NLunc, plasma sample preparation started directly with the first basic LLE, skipping the enzymatic hydrolysis. If concentrations determined in plasma samples obtained after NDiol supplementation exceeded the defined working ranges, 0.25 ml of respective specimens was diluted using blank plasma [1:1 (v/v)] before reapplied sample preparation.
Analysis by GC/MS. Gas chromatography/mass spectrometry (GC/MS) analysis was performed with a quadrupole mass selective detector HP 5973 coupled to an HP 6890 gas chromatograph (Agilent Technologies, Waldbronn, Germany). An HP 5-crosslinked methyl silicone capillary column (length, 17 m; i.d., 0.25 mm; film thickness, 0.25 μm) was used, with helium as carrier gas at a constant flow rate of 1.0 ml/min. A 2-μl aliquot of sample was injected onto the GC column in the splitless mode. The temperature program started at 100°C, increased by 40°C/min up to 190°C, 5°C/min up to 240°C, and finally 40°C/min up to 320°C and rest for 3 min. Injection port and transfer line were heated to 300°C. Data acquisition was performed using electron impact ionization at 70 eV, and selected ion monitoring mode with dwell times of 20 ms for each ion was used. Two fragment ions of each target analyte were selected for qualitative and quantitative determination (Table 1). To facilitate and optimize quantitation results, three stably deuterated compounds were used as internal standards (ISTDs): d3-NDiol, d3-NL, and d3-NE (Fig. 2, A–C) were used for isotope-dilution mass spectrometry of NDiol, NL, NA, and NE, respectively. In Table 1, characteristic fragment ions of target analytes and ISTDs are listed, the bold mass-to-charge values of which represent ions used for quantification purposes. Peak areas of deuterated ISTDs were corrected by subtracting the isotope signals of corresponding unlabeled analytes. As depicted in Fig. 3, informative fragment ions are influenced by deuterium labeling, e.g., the molecular ion M+ at m/z 420 and (M+-15) at m/z 405 are incremented by 3 U to m/z 423 and 408, respectively. Moreover, fragment ions resulting from cleavages of the steroid nucleus such as m/z 129 and 142 (Table 1) demonstrate the diagnostic character of electron ionization mass spectra used for qualitative and quantitative determination of target analytes. Although the ion at m/z 129 was generated from the steroidal D-ring under hydrogen rearrangement as substantiated by the presence of its deuterated counterpart at m/z 131 in the case of d3-NDiol, the fragment at m/z 142 resulted from the A-ring as reported in the literature earlier (Thevis and Schänzer, 2005).
Characteristic ions of steroids used for qualitative and quantitative determination
All steroids were analyzed as bis-TMS derivatives. Bold values represent ions used for quantitation purposes.
Validation of the Analytical Method.Calibration curves. A calibration curve was generated for the quantification of each analyte. Therefore, male control blank plasma was fortified with respective analytes before passing sample preparation. Samples were run in duplicates at six different nonzero concentrations for all standard curves to verify linearity for all analytes within the defined working ranges (Table 2).
Validation parameters and results for plasma total concentrations (conjugated and unconjugated) of NDiol, NL, NA, NE, and unconjugated NL (NLunc)
Accuracy and precision. Accuracy and precision were determined by replicate analysis of samples containing known amounts of the analytes. Depending on the extent of the working ranges, accuracy and precision were measured using five determinations each of up to three different concentration levels (Table 2).
Lower limit of quantification. The lower limits of quantification (LLOQ) were established using five samples for each analyte. At these levels, analyte peaks should be identifiable, discrete, and reproducible with a precision of 20% and accuracy of 80 to 120% (U.S. Food and Drug Administration, Guidance for Industry Bioanalytical Method Validation, Center for Drug Evaluation and Research, http://www.fda.gov/cder/guidance/index.htm).
Recovery. Recovery of all analytes were determined as follows: six blank plasma samples were spiked with defined amounts of NDiol, ND, NA, and NE (Table 2) before sample preparation, and another six blank plasma samples were extracted according to the described protocol. Before the last drying and subsequent derivatization step, nonspiked blank plasma samples were fortified with respective norsteroids, and all samples were enriched with 20 μl of the ISTD mixture. Recoveries were calculated by comparison of mean peak area ratios of analytes and ISTD of samples fortified before and after sample preparation. Linearity, LLOQ, accuracy, precision, and recovery were determined for total plasma steroid concentrations (unconjugated plus conjugated steroids) of NDiol, NL, NA, and NE as well as for NLunc.

Electron ionization mass spectra of the target analyte NDiol bis-TMS (A; mol. wt., 420) and its deuterated analog d3-NDiol bis-TMS (B; mol. wt., 423). The molecular ion as well as characteristic fragment ions such as m/z 330 and 240 differ by 3 U because of deuterium labeling, whereas m/z 129, resulting from the steroidal D-ring, is shifted to m/z 131 by two deuterium atoms only. The ion at m/z 142 remains constant, since it is suggested to originate from the unlabeled A-ring.
Pharmacokinetic and statistical evaluation. The pharmacokinetic parameters tmax (time of peak plasma concentration) and Cmax (peak plasma drug concentration) were calculated for NDioltot, NLtot, NAtot, NEtot, and NLunc for each subject. Individual values for the area under the plasma level-time curve (AUC) were determined by the trapezoidal rule method. Calculations resulted directly from the measured plasma concentration data without curve fitting. Variables for tmax were analyzed by nonparametric Wilcoxon signed rank test. Data for Cmax and AUC were tested for normal distribution (Kolmogorov-Smirnov test) and were compared between both treatment groups (capsule and sublingual tablet) by means of paired t test. All parameters were tested for significant differences at the 5% level, and p values were adjusted by Bonferroni correction. The programs BIAS for Windows (8.2) and R (R Development Core Team, 2005) were used for the statistical analysis.
Results
GC/MS analyses of plasma samples enabled the determination of all target analytes as depicted exemplarily in Fig. 4. The specimen was collected 1 h after administration of a sublingual tablet (25 mg of NDiol), and NDiol (Fig. 4A) as well as the metabolites NL (NLtot, Fig. 4B; NLunc; Fig. 4D), NA, and NE (Fig. 4C) were detected using the established approach at concentration levels ranging from 1.8 to 109.2 ng/ml.
Validation of the Analytical Method. Validation results are summarized in Table 2. Linearity was proven for all analytes within the defined working ranges. The lowest levels of the working ranges represent the respective LLOQ. Results for calibration curves, LLOQ, accuracy, and precision met requirements of the Guidance for Industry for Bioanalytical Method Validation (U.S. Food and Drug Administration, Center for Drug Evaluation and Research, http://www.fda.gov/cder/guidance/index.htm).
Plasma Concentrations of Norsteroids after Administration of a 100-mg NDiol Capsule.Plasma total concentrations (unconjugated and conjugated steroids). After oral administration of a 100-mg capsule, NDioltot was quantified in low amounts up to 2.3 ng/ml (Fig. 5A). Concentrations of NDioltot were detected during the entire monitoring period (8 h), peaked out between 1 and 8 h after application, and returned to baseline levels within 24 h. Only the plasma samples of one volunteer did not contain NDioltot. NDioltot concentrations of another volunteer, referred to as V8 hereafter, remained at baseline approximately 4 h before increasing during a subsequent 4-h period. After 24 h, plasma level concentrations of V8 and yet another volunteer still remained above LLOQ, determined at 0.6 and 1.0 ng/ml, respectively. NLtot was detected in plasma samples of the volunteers up to 8 h after administration. Plasma samples of the particular volunteer, which already showed no NDioltot, did also not contain NLtot. Maximum values of the remaining volunteers varied between 1.6 and 8.8 ng/ml (Fig. 5B). The plasma concentration course of V8 remained at baseline approximately 4 h before increasing after NDiol administration. Oral ingestion of a 100-mg capsule of NDiol resulted in maximum total plasma concentrations of NAtot and NEtot, ranging from 53.4 to 461.7 ng/ml (Fig. 5C) and 22.0 to 44.9 ng/ml (Fig. 5D), respectively. For approximately 4 h, plasma level concentrations of these metabolites remained at baseline values for V8 increasing rapidly during the subsequent 4-h period, especially for NAtot. Plasma levels of NAtot and NEtot decreased slowly, and 24 h after the administration, considerable amounts up to approximately 30 ng/ml for both compounds were still detected.

GC/MS analysis of a plasma sample collected 1 h after administration of 25 mg of NDiol (sublingual tablet). The extracted ion chromatograms contain target analytes (solid lines) and respective deuterated internal standards (dotted lines): 1.8 ng/ml NDiolto (A), 11.9 ng/ml NLtot (B), 109.2 ng/ml NAtot and 20.7 ng/ml NEtot (C), and 2.2 ng/ml NLunc (D).
Plasma concentrations of unconjugated nandrolone. After ingestion of one Norandrodiol capsule containing 100 mg of NDiol, only very low amounts of NLunc were detected in plasma samples of the volunteers. In fact, values of only one volunteer exceeded the limit of quantification of 0.5 ng/ml, as determined at 0.7 and 0.6 ng/ml, 45 and 60 min after administration, respectively.

Plasma total concentrations of NDioltot (A), NLtot (B), NAtot (C), and NEtot (D) after administration of a capsule containing 100 mg of NDiol (eight volunteers). For clarity purposes, V8 is shown using a dotted line.

Plasma concentrations of NDioltot (A), NLtot (B), NAtot (C), and NEtot (D) after administration of a sublingual tablet containing 25 mg of NDiol (eight volunteers).

Plasma concentrations of NLunc after administration of a sublingual tablet containing 25 mg of NDiol (eight volunteers).
Plasma Concentrations of Norsteroids after Administration of a 25-mg NDiol Sublingual Tablet.Plasma total concentrations (unconjugated and conjugated steroids). Administration of NDiol by the sublingual formulation resulted in fast absorption of the parent compound, which was detected in plasma samples of all volunteers. Maximum concentrations were determined in a range from 1.6 to 4.3 ng/ml for each volunteer (Fig. 6A). Concentrations peaked out within 45 min and declined to baseline levels no later than 4 h after administration. Already 10 min after the application of Cyclo-Nordiol, the formation of NL was detected in plasma samples of all volunteers. Maximum plasma total concentrations of NLtot varied between 4.4 and 20.2 ng/ml and were reached within 1 h after application (Fig. 6B). In addition, concentrations of the main metabolites NA and NE increased at an early stage. Maximum values for NAtot varied between 41.8 and 169.2 ng/ml (Fig. 6C) and for NEtot between 12.0 and 72.2 ng/ml (Fig. 6D). Trace amounts of NAtot were still detected 24 h after administration but remained below LLOQ.
Plasma concentrations of unconjugated nandrolone. Ten minutes after sublingual administration of 25-mg NDiol sublingual tablets, considerable amounts of NLunc in plasma samples of all volunteers were quantified. Plasma concentrations of each volunteer peaked within 30 min after application and were determined between 3.2 and 5.7 ng/ml (Fig. 7). Although concentrations fell below the lower limit of quantification of 0.5 ng/ml, NLunc was still detected in all specimens 3 h after application.
Statistical and Pharmacokinetic Evaluation. Mean values (±S.E.) of Cmax, tmax, and AUC were calculated for NDioltot, NLtot, NAtot, NEtot, and NLunc as obtained from eight volunteers after administration of one 100-mg NDiol capsule and one 25-mg NDiol sublingual tablet, respectively (Table 3).
Summary of pharmacokinetic evaluation
Discussion
In the current investigation, we compared metabolite profiles in plasma resulting from administrations of two differently formulated NDiol products. In contrast to urine analysis, blood analysis has enabled the detection of the applied prohormone and the intermediately formed NL, in addition to the main metabolites NA and NE.
After consumption of a 100-mg NDiol capsule, NDioltot and NLtot were determined after enzymatic hydrolysis in plasma samples of seven of eight volunteers in low amounts (0.8–2.3 and 1.6–8.8 ng/ml, respectively; Fig. 5). In plasma samples of all volunteers, NA and NE were identified as major metabolites, whereas NLunc (i.e., without hydrolysis) was quantified in low amounts near the LLOQ in one case only (0.7 ng/ml, data not shown). The deviant course of the concentration curves of all quantified norsteroids in plasma samples of V8 might result from a delayed dissolution of the capsule.
Concentration curves after administration of 25-mg NDiol sublingual tablets were characterized by a fast absorption of the prohormone as well as a fast increase of its metabolites in samples of all volunteers. Furthermore, NLunc was detected and quantified in considerable quantities in plasma samples of all subjects (3.2–5.7 ng/ml).
Considering the fact that the administration of sublingual tablets applies only one-fourth of the dose administered when using NDiol capsules, this drug formulation leads to significantly higher mean peak concentrations for NDioltot and NLtot. Even though only low amounts of the parent compound were determined in plasma samples of both test groups (capsule and sublingual tablet), demonstrating no significant difference regarding mean AUC (p = 0.1977), the mean Cmax value for NDioltot is significantly higher after administration of the 25-mg NDiol sublingual tablet (p = 0.0001). In addition, plasma NLtot concentrations reached a mean value of 11.0 ng/ml (±6.4), which accounts for nearly the 3-fold amount registered after ingestion of the 100-mg NDiol capsule (p = 0.0083), but the mean AUC for NLtot is 2 times higher in the 100-mg capsule test group (p = 0.0324). No significant differences for Cmax of the main metabolites NA and NE have been observed (p = 0.3333 and 0.3692, respectively). Regarding mean AUCs, values for both NAtot and NEtot are significantly higher after administration of NDiol capsules compared with the sublingual formulation (p = 0.048 and 0.0001, respectively). Although only low concentrations of NLunc in plasma samples of one volunteer were detected after capsule administration, sublingually administered NDiol was effective in raising plasma NLunc levels, determined at 4.4 ng/ml (±1.0). Furthermore, sublingual administration of NDiol produced uniform hormonal responses and reduced mean time to peak concentrations (tmax) as well as fast decrease in plasma concentrations for all analytes compared with oral administration (Figs. 5, 6, 7). The tmax values for NDioltot, NLtot, NAtot, and NEtot (p = 0.009, 0.0533, 0.0624, and 0.0083, respectively) were significantly different only for NDioltot and NEtot.
These findings result from different absorption kinetics because of the different drug formulations. Initially, prohormones such as NDiol have widely been used in form of capsules or pills. Manufacturers introduced sublingual formulations of prohormones to the supplement market intending to improve effectiveness of their products. This pharmaceutical form should prevent prohormones from assumed hepatic catabolism if consumed orally. Sublingual tablets are designed for drug release under the tongue and are used for compounds, which are able to penetrate mucosal membranes. In sublingual tablets (or “lozenges” as labeled by the manufacturer), hydroxypropyl-β-cyclodextrin forms an inclusion complex with NDiol to forward dissolution. Compounds absorbed through the oral mucosa are distributed within the body before the first hepatic metabolism. As a consequence, sublingual application may provide better bioavailability and a shorter onset time over oral administration for drugs with noticeable first-pass effect.
To evaluate whether concentrations of NLunc generated from prohormones are pharmacologically relevant, pharmacokinetic investigations regarding NL-containing therapeutics have been considered. These drugs have generally been marketed as depot injections and not for oral administration. The single i.m. application of 100 mg of NL decanoate to healthy male volunteers resulted in mean peak plasma concentrations of 4.3 ng/ml NL (2.9–6.9 ng/ml) (Bagchus et al., 2005), and weekly injections of 200 mg of NL-3-(p-hexoxyphenyl)-propionate for 10 weeks yielded NL plasma levels up to 5.5 ng/ml (Belkien et al., 1985). Here, plasma testosterone suppression was considered as an important indicator for the pharmacological activity of NL, and testosterone levels did not recover from suppressive effects until NLunc concentrations declined to 0.3 to 1.2 ng/ml (Belkien et al., 1985; Knuth et al., 1985; Minto et al., 1997). Hence, this concentration range of NLunc can be regarded as the minimum effective concentration of the drug that will result in a pharmacological effect. Sublingual uptake of 25 mg of NDiol resulted in maximum plasma levels of NLunc between 3.7 and 5.7 ng/ml; i.e., all volunteers have been exposed to pharmacologically relevant plasma concentrations of NLunc for at least 2 h if compared with acute therapeutic nandrolone application. Although these concentration levels remained for only 2 to 3 h, pharmacological effects cannot be ruled out, especially considering a multiple intake of the respective supplement.
To the best of our knowledge, this study is the first reporting on the in vivo conversion of nandrolone prohormones into nandrolone. Related studies examined the acute effect of orally administered testosterone prohormones such as androstenedione and androstenediol, which did not result in uniform findings concerning the elevation of plasma testosterone concentrations of young healthy men (King et al., 1999; Brown et al., 2000; Earnest et al., 2000, Leder et al., 2000). In accordance to our results, an increase of plasma testosterone concentrations after sublingual androstenediol intake was reported (Brown et al., 2002), demonstrating the effectiveness of this route of drug administration.
Conclusion
The observed plasma NLunc concentrations after application of NL prohormones as determined in the present study are alarming, since NDiol in particular was marketed as nutritional supplement and may have been (mis)used in amateur and professional sports. Our findings suggest that NDiol supplementation may have exposed the users to unpredictable health risks as its in vivo conversion to the active compound NL was demonstrated. Moreover, the rationale for prohibiting prohormones such as NDiol in sports was substantiated since the prohibited compound NL was generated in addition to the common metabolites NA and NE.
Acknowledgments
We are grateful to Professor Dr. Petra Platen, University of Bochum, Institute for Sports Medicine and Sports Nutrition, Bochum, Germany, for medical attendance.
Footnotes
-
This project has been carried out with support from WADA.
-
Article, publication date, and citation information can be found at http://dmd.aspetjournals.org.
-
doi:10.1124/dmd.106.010165.
-
ABBREVIATIONS: NL, 17β-hydroxy-estr-4-en-3-one (nandrolone); NA, 3α-hydroxy-5α-estran-17-one (19-norandrosterone); NE, 3α-hydroxy-5β-estran-17-one (19-noretiocholanolone); WADA, World Anti-Doping Agency; ND, estr-4-ene-3,17-dione (19-norandrostenedione); NDiol, estr-4-ene-3β,17β-diol (19-norandrostenediol); unc, unconjugated; p.a., pro analysi; d3-NE, 3,4,5-2H3-3α-hydroxy-5β-estran-17-one; d3-NDiol, 16,16,17-2H3-estr-4-ene-3β,17β-diol; d3-NL, 16,16,17-2H3-17β-hydroxy-estr-4-en-3-one; tot, total (conjugated plus unconjugated); LLE, liquid-liquid extraction; GC/MS, gas chromatography/mass spectrometry; ISTD, internal standard; LLOQ, lower limits of quantification; AUC, area under the plasma level-time curve; TMS, trimethylsilyl.
- Received March 14, 2006.
- Accepted May 17, 2006.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}