





Abstract
Ciclesonide is an inhaled corticosteroid, administered as a prodrug via a metered-dose inhaler. Following deposition in the lung, ciclesonide is hydrolysed by esterases to form the pharmacologically active metabolite desisobutyryl-ciclesonide (des-CIC). Formation of des-CIC, as well as reversible esterification of des-CIC with fatty acids, has been demonstrated in vitro. The aim of this study was to investigate the in vivo metabolism of ciclesonide in the human lung.
This single-dose, open-label, nonrandomised study was performed in 20 patients undergoing planned lung surgery for treatment of malignant pulmonary lesions. Patients inhaled a single dose of 1,280 μg ciclesonide at various time-points between 2 and 24 h prior to lung tissue resection. The concentration of ciclesonide, des-CIC and fatty acid conjugates of des-CIC in tissue samples was determined. Serum samples for pharmacokinetic analysis were taken at several time-points after inhalation.
The pharmacokinetics in serum indicated that the inhalation by the patients was adequate. Metabolites (des-CIC, des-CIC oleate and des-CIC palmitate) were detected in the resected central and peripheral lung tissues. A substantial portion of ciclesonide was already activated to des-CIC at the first time-point of tissue analysis.
Activation of ciclesonide and formation of des-CIC fatty acid conjugates was confirmed in vivo in the human lung.
Asthma is one of the most common chronic inflammatory disorders of the airways and is characterised by airway obstruction, inflammation and hyperresponsiveness resulting from complex interactions among inflammatory cells, mediators, and the cells and tissues of the airways 1, 2. International and national treatment guidelines recommend the use of inhaled corticosteroids (ICS) as first-line therapy for patients with asthma 3, 4.
Ciclesonide is a novel ICS administered as a prodrug via a metered-dose inhaler using hydrofluoroalkane (HFA) as the propellant. It is available as Alvesco® (Nycomed GmbH, Kostanz, Germany) in many markets. Ciclesonide is converted to the active metabolite desisobutyryl-ciclesonide (des-CIC), by esterases that cleave isobutyrate at the C21 position 5–7. Des-CIC has a much higher affinity for the glucocorticoid receptor than ciclesonide (∼100 times higher) 5, 8. Alvesco® has a high pulmonary deposition of 52% 9, 10. Both oropharnygeal deposition of ciclesonide and activation of ciclesonide in the oropharynx to des-CIC are low 10–12.
In vitro studies in human tissue and in vivo studies in rats have reported that des-CIC forms reversible conjugates with fatty acids, which are pharmacologically inactive and do not bind to the glucocorticoid receptor 7, 13–15. The findings regarding the metabolism of CIC derived from in vitro and animal studies have yet to be confirmed by in vivo studies in human subjects. It was the aim of the present study to investigate for the first time the in vivo deposition and metabolism of ciclesonide by applying a comprehensive analysis of CIC, des-CIC, and its reversible conjugates in central and peripheral human lung tissue.
METHODS
Subjects
Inclusion criteria
Male and female patients undergoing elective lung surgery for malignant pulmonary lesions, aged 18–70 yrs were eligible for inclusion in the study. Patients had to demonstrate an acceptable inhalation technique at screening and have a forced expiratory volume in 1 s (FEV1) ≥70% predicted. In addition, the therapeutic surgical strategy for the underlying disease had to require the removal of lung tissue.
Lung tissue prepared for pharmacological analysis in this study had to be ventilated prior to resection (i.e. without relevant proximal bronchial obstruction), vital at the time of resection, and noncancerous. The tissue used for analysis was removed for therapeutic reasons only and was not required for any other therapeutic or diagnostic procedures.
Exclusion criteria
Patients with diseases contraindicating the use of ICS (e.g. active pulmonary tuberculosis or relevant fungal, bacterial or viral infections of the lower respiratory tract), those with a history of allergic reactions to ICS or HFA-solution aerosols, and those participating in a clinical study ≤30 days before the start of the current study were excluded. Pregnant females, nursing mothers or females of childbearing potential who were not using a medically acceptable and reliable method of contraception for the entire study duration were not eligible to participate.
Ethics
The study was performed in compliance with the International Conference on Harmonization (ICH) Guidelines for Good Clinical Practice (ICH Consolidated Guideline E6) and the Declaration of Helsinki in its revised form (Somerset West, South Africa, October 1996). The protocol was approved by the Independent Ethics Committee at the Faculty of Medicine of Heidelberg University. All patients gave written informed consent.
Study design
This was an open-label, single-dose, nonrandomised pilot study. Patients underwent a screening examination 2–7 days prior to the treatment day. On the treatment day, patients inhaled a single dose of ciclesonide (Alvesco®) (1,280 μg ex-actuator; equivalent to 1,600 μg ex-valve; to be inhaled by eight puffs of 200 μg within 4 min) 2–24 h prior to scheduled surgical removal of the lung tissue. The time between inhalation of ciclesonide and scheduled surgical removal (i.e. clipping the resected tissue from the remaining part) of the lung tissue was planned to be divided into four groups of five patients each, to cover the complete period between 2 and 24 h. The intended grouping was >2–4 h, >4–8 h, >8–16 h and >16–24 h.
In addition, three patients did not take any study medication but donated lung tissue as controls for bioanalytic testing of matrix effects. Patients who received ciclesonide underwent a post-study examination 3–5 days after receiving treatment.
All measures that were required for the pre-operative management of the patient were performed irrespective of the current study, according to the medical needs of the patient. Concomitant medication for the adequate clinical management of the patient was allowed.
Serum samples
To assess adequate inhalation, blood samples for pharmacokinetic analysis were taken pre-dose and at 0.75, 1.5, 3, 6, 12 and 24 h post-dose. Blood (4 mL) was sampled into nonheparinised serum monovettes and immediately stored at 2–8°C for 60–90 min to allow clotting. Samples were then centrifuged (2,000×g, 4°C) for 10 min to obtain serum, which was transferred into polypropylene tubes. All samples were stored at -20°C until further analysis.
Lung tissue preparation
The lung tissue sample for analyses was excised from the surgical lung specimen immediately after resection. The sample had to measure at least 2.5×2.5×2.5 cm (equivalent to a volume of ∼16 mL). If a single piece of tissue of this size was not available, several smaller pieces from one anatomical area were dissected until a total volume of ∼16 mL was reached. A central airway had to be identified within the sample and the bronchial tree was dissected removing the adjacent tissue, as long as the small bronchi could be clearly identified macroscopically. For the purpose of this study, a central airway was defined as having a diameter of ∼1–3.5 mm in order to start the dissection with cartilaginous airways, which helps to clearly identify bronchi within the sample. Peripheral airways with cross-sections <1 mm, together with adjacent lung tissue, represented the peripheral lung tissue.
All lung tissue samples (two or three aliquots per sample) were stored at -80°C after dissection until further analysis (pharm-analyt Labor GmbH, Baden, Austria). Lung samples were weighed, cut into smaller pieces, thawed, homogenised in ethanol and extracted in cold conditions (8–15°C). The samples were centrifuged (3,000×g) and extracts were collected.
Histological specimens of lung tissue from patients treated with the study drug and those in the control group were also prepared and stained with haemalaun and eosin.
Analysis of ciclesonide and metabolites
For the lung samples, the concentrations of ciclesonide, des-CIC and the two fatty acid conjugates of des-CIC (des-CIC oleate and des-CIC palmitate) were determined using high-performance liquid chromatography with tandem mass spectrometry (LC-MS/MS). The analytical method for the tissue samples was established at pharm-analyt Labor GmbH using lung tissue samples from pigs, as well as from patients in the control group who received no ciclesonide. For des-CIC in serum, analyses were performed by Nycomed GmbH. The analytical methods are based on validated LC-MS/MS methods used previously in other pharmacokinetic studies 16–19.
Due to the different molecular weights of the metabolites, a comparison based on molar concentration was considered most appropriate. The lower limits of quantitation (LLOQs), based on tissue samples of 0.5 g, were 0.563 pmol·g−1 for ciclesonide, 0.644 pmol·g−1 for des-CIC, 0.136 pmol·g−1 for des-CIC oleate and 0.0424 pmol·g−1 for des-CIC palmitate. Dilution factors were taken into account when a sample of <0.5 g was provided.
Safety
Safety and tolerability assessments were based on adverse events reported during the entire study, clinical laboratory values, lung function tests (spirometry), physical examinations, ECGs, blood pressure, pulse rate and body temperature. Vital signs were measured as close as possible to the time-points scheduled for the pharmacokinetic measurements.
Pharmacokinetic evaluation
The sample size of 20 patients receiving ciclesonide and three control patients was chosen on grounds of feasibility. The primary variables in this study were the lung-tissue concentrations of ciclesonide, des-CIC and the fatty acid conjugates of des-CIC. The total concentration of ciclesonide-related compounds (sum of ciclesonide, des-CIC, des-CIC oleate and des-CIC palmitate) was also calculated, and compared between central and peripheral lung tissue. The following pharmacokinetic parameter characteristics were also assessed for the active metabolite, des-CIC, based on the concentrations in serum at 0.75, 1.5, 3, 6, 12 and 24 h post-dose: maximum serum concentration (Cmax), time to reach Cmax (tmax), terminal elimination half-life (t1/2) and area under the serum concentration–time profile extrapolated to infinity (AUC0–inf). AUC0–inf was calculated using the trapezoidal formula up to the last sampling time with a concentration above the LLOQ (10 pg·mL−1) and extrapolated to infinity using standard techniques. Cmax and tmax were obtained directly from the serum concentration–time profiles. The pharmacokinetic evaluation was performed using WinNonlin professional, Version 4.1 (Pharsight Corporation, Mountain View, CA, USA). All variables were analysed in a descriptive manner using summary statistics including mean, sd or sem. Secondary safety variables were analysed in a descriptive manner.
RESULTS
Subjects
A total of 20 patients (15 males and five females) with a median age of 58 yrs were included in the study (table 1). All of the patients were undergoing surgery for pulmonary malignant lesions (lung cancer, n = 17; pulmonary metastases of breast cancer, n = 2; pulmonary metastases of sarcoma, n = 1) and underwent anatomical segmentectomy or lobectomy. All patients were Caucasian and had a median height of 174 cm and a median weight of 74 kg. The majority of patients (n = 19) were ex- (n = 11) or current (n = 8) smokers. 10 patients were assigned to have mild to moderate chronic obstructive pulmonary disease according to their medical records. All patients had an FEV1 ≥70% predicted.
Assay performance
Serum concentrations of des-CIC were determined using a previously validated bioanalytical method. The LLOQ was 10 pg·mL−1. The interbatch precision and accuracy of the quality control (QC) samples for des-CIC in serum were 1.88–6.52% and 97.3–97.9%, respectively.
The bioanalytical evaluations of ciclesonide, des-CIC and the oleate and palmitate of des-CIC in lung tissue were performed using a validated LC-MS/MS method (LLOQ provided previously). The interbatch precision and accuracy results of the QC samples for all analytes in tissue were 2.79–5.44% and 93.9–105.6%, respectively.
Pharmacokinetics
The pharmacokinetic evaluation focused on the pharmacologically active metabolite des-CIC, which is the major metabolite in serum. The Cmax of des-CIC was attained between 0.75–1.5 h after ciclesonide inhalation, and the mean Cmax of des-CIC was 3.29 pmol·mL−1 (1.55 μg·L−1). Serum concentrations of des-CIC decreased with a mean t1/2 of 5.7 h (table 2).
Lung tissue
There were no interfering matrix effects in the bioanalysis as ciclesonide, des-CIC, des-CIC oleate and des-CIC palmitate were not detectable in the control samples from the three patients who did not inhale ciclesonide. Histological evaluation of all peripheral lung tissue samples revealed normal lung parenchyma.
For patients who had inhaled ciclesonide, a total of 39 central and peripheral lung tissue samples were available for the bioanalysis (no central tissue sample was obtained in one patient dosed 2.08 h prior to surgery), and three aliquots per sample were obtained for 19 patients. Because the concentrations of analytes in the aliquots were below the LLOQ in some cases, median concentrations were provided for the corresponding sample.
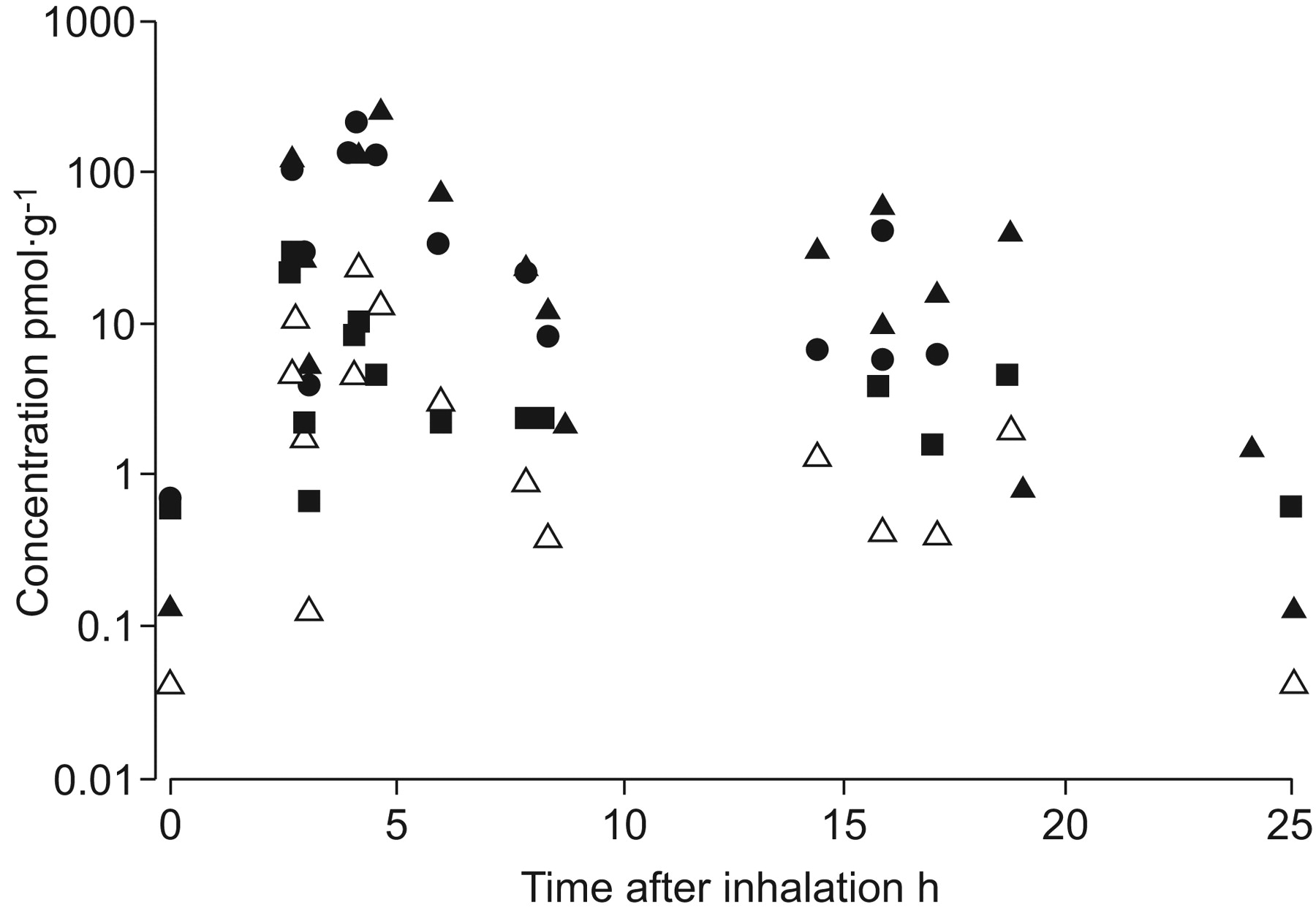
Ciclesonide, des-CIC, des-CIC oleate and des-CIC palmitate were detectable in the tissue samples and the individual results are given in figure 1 and figure 2.
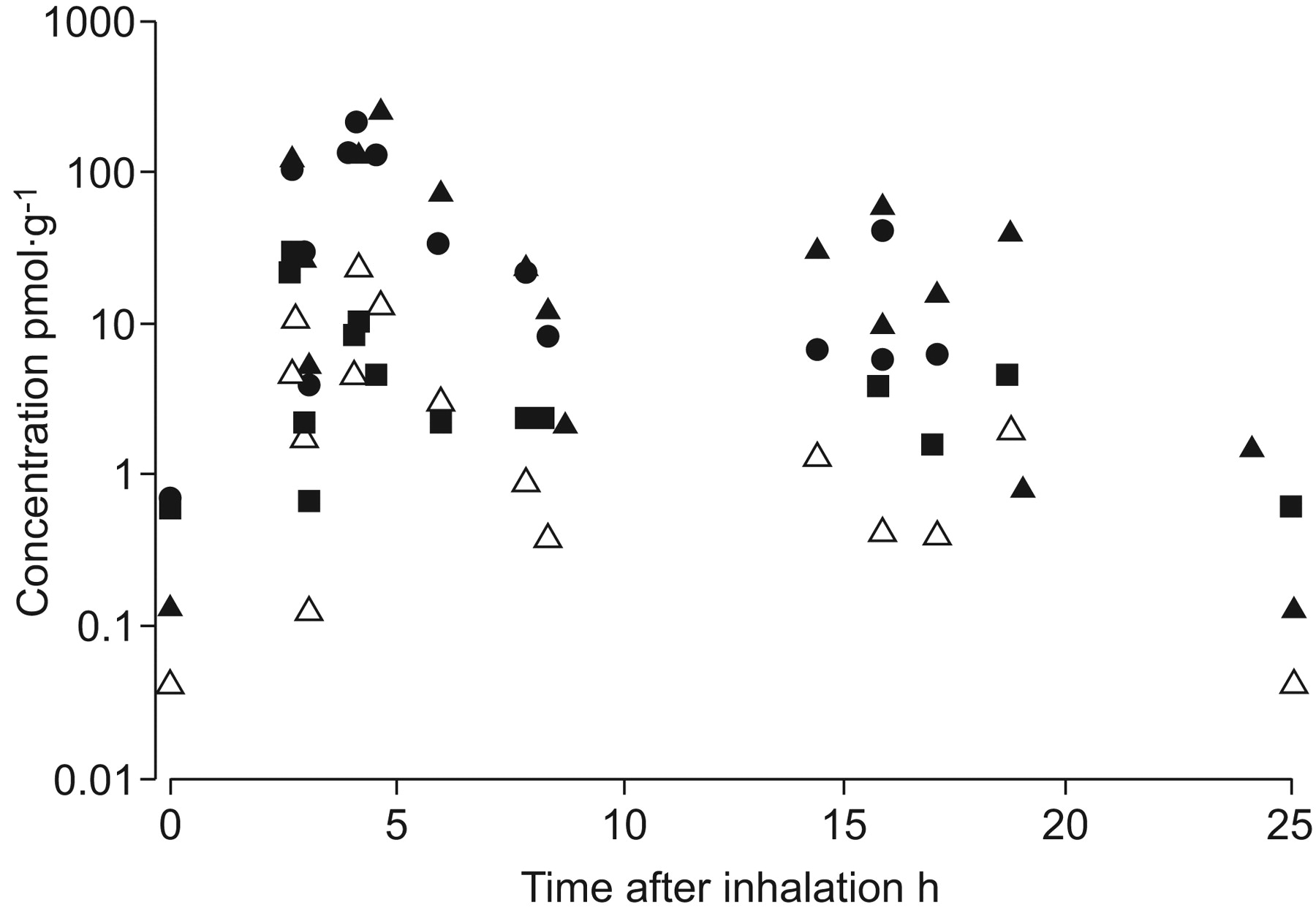
Concentrations of ciclesonide (CIC; ▪), and its active metabolite desisobutyryl-CIC (des-CIC; •) and fatty acid ester conjugates (des-CIC oleate (▴) and des-CIC palmitate (▵)) in central lung tissue. The lower limit of quantitation of the compounds is provided for illustration at 0 and 25 h.
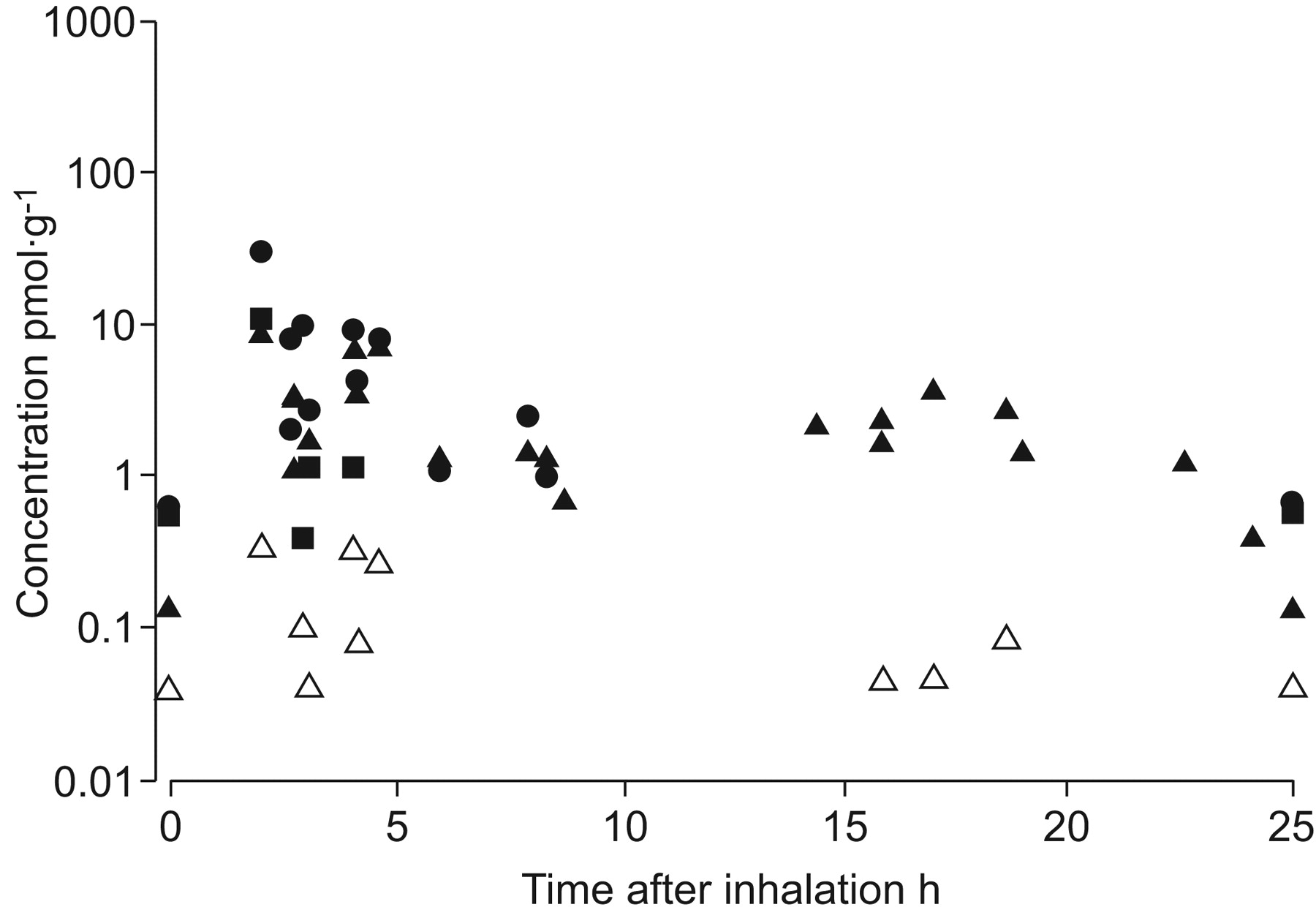
Concentrations of ciclesonide (CIC; ▪), and its active metabolite desisobutyryl-CIC (des-CIC; •) and fatty acid ester conjugates (des-CIC oleate (▴) and des-CIC palmitate (▵)) in peripheral lung tissue. The lower limit of quantitation of the compounds is provided for illustration at 0 and 25 h. The lung resections of two patients were performed at the same time (4.17 h following inhalation); therefore, a slight offset for different time-points in these patients was used for better illustration.
A substantial proportion of ciclesonide was hydrolysed to des-CIC even at the earliest available time-point of 2.08 h after inhalation of ciclesonide. In peripheral lung tissue, the highest concentration of des-CIC (30.2 pmol·g−1) was measured at this time-point. In almost all samples with detectable des-CIC concentrations, the level of the metabolite was higher than that of the parent compound. The concentrations of ciclesonide were below the LLOQ in the majority of central lung tissue samples collected ≥14 h after inhalation. The same was true for all samples of peripheral lung tissue obtained ≥4.5 h after inhalation. After 8 h, des-CIC oleate was the main metabolite in both the central and peripheral lung tissue samples. At least one of the metabolites of ciclesonide was present in the lung tissue samples at all study time-points up to 24 h.
The distribution of time-points of resection following inhalation was well balanced within the investigational period, as five patients were included per group (>2–4 h, >4–8 h, >8–16 h and >16–24 h). The earliest time-point was 2.08 h and the latest time-point after inhalation was 24.08 h. Table 3 presents the median concentrations of ciclesonide and its metabolites in lung tissue.
After inhalation of 1,280 μg ciclesonide, the concentrations of ciclesonide and its metabolites (des-CIC, des-CIC oleate and des-CIC palmitate) were higher in the central airway tissue than in the peripheral lung tissue. Des-CIC and des-CIC oleate were the main metabolites in both lung areas. The levels of des-CIC palmitate were considerably lower than those of des-CIC oleate overall and in both lung areas (table 3).
Comparison of total ciclesonide-related compounds
Overall, higher concentrations of total ciclesonide-related compounds were found in the central airways compared with peripheral lung tissue. No time-dependent changes were noted in the ratio of total concentrations in central to peripheral lung tissue during the 24 h after inhalation of ciclesonide (fig. 3). Regression analysis of the two sets of data resulted in apparent t1/2 of the total ciclesonide-related concentrations of ∼5 h in the lung tissue.

{kind=link}
{kind=link}
{kind=link}
Total concentrations (sum of the concentrations for ciclesonide, desisobutyryl-ciclesonide, oleate and palmitate) in central (▪) and peripheral (•) lung tissue. The corresponding linear regression lines are shown (—: central; ---: peripheral).
The concentration of des-CIC in serum decreased similarly over time, resulting in a t1/2 of 5.7 h (table 2); however, the concentrations were lower. The mean concentration of the major metabolite des-CIC in serum at 1.5 and 24 h was 2.5 and 0.1 pmol·mL−1, respectively.
Safety analysis
A total of seven treatment-emergent adverse events (TEAEs) (atrial fibrillation, acute respiratory distress syndrome, pneumonia, sepsis, enteritis, QTc interval prolongation and pyothorax) were reported by four patients. Three TEAEs were mild or moderate in intensity and four (in two patients) were severe. In all cases, TEAEs were determined to be unrelated to the study medication. None of the TEAEs led to study discontinuation. Laboratory abnormalities and findings at physical examination were surgery-related and assessed by the investigators not to be clinically relevant.
DISCUSSION
After inhalation of a single dose of 1,280 μg ciclesonide by patients undergoing elective lung surgery, ciclesonide was rapidly hydrolysed to des-CIC in both central airways and peripheral lung tissue. Des-CIC and des-CIC oleate were the main metabolites in both compartments, and at least one of the metabolites of ciclesonide (des-CIC, des-CIC oleate or des-CIC palmitate) was present in the lung tissue samples at all study time-points up to 24 h. The results are of relevance as the study was performed in humans who inhaled ciclesonide and tissue samples of the target organ of the drug were taken from living patients. These in vivo findings confirm the two major metabolic pathways of ciclesonide in the human lung: the rapid, on-site conversion of ciclesonide to des-CIC and the conjugation of des-CIC with fatty acids, in particular oleic acid. Such findings have previously been shown in vitro in human tissue and in vivo in animals 13–15.
A 1,280 μg dose of ciclesonide was selected in the current study as this was expected to be sufficient for detection in the pharmacokinetic analysis. Previous studies have indicated the safety of 1,280 μg·day−1 ciclesonide 20, 21. As ciclesonide was always inhaled ≥2 h prior to anaesthesia, the absorption of the drug is assumed not to be influenced by the anaesthetics. The pharmacokinetic profiles of serum des-CIC concentrations measured over time indicated that drug inhalation by patients (of whom, the majority were ex- or current smokers) was adequate; the AUC of des-CIC in this study was 6.68 μg·h·L−1 following a single dose of 1,280 μg ciclesonide. The dose-adjusted AUC values in healthy subjects were in the range of 4.11 μg·h·L−1 and 7.32 μg·h·L−1 16, 17. The pharmacokinetic and pharmacodynamic properties of inhaled ciclesonide have been described in recent publications 22–24.
Total lung tissue concentrations of ciclesonide, des-CIC and the fatty acid conjugates of des-CIC were higher in the central airways than in the peripheral-lung tissue. However, the amount of the drug that reached the peripheral lung was substantial, which is consistent with previous findings of high peripheral lung deposition of ciclesonide 10. Overall, 55.8% of the deposited dose was found in the peripheral lung that represented ∼75% of the lung volume. Effects of ciclesonide on small airways were recently demonstrated in a clinical study 25. The elimination of the total concentrations was similar in peripheral and central lung tissue. Therefore, the ratio between peripheral and central lung appeared to be stable. At all time-points, the total ciclesonide-related concentrations in the central and peripheral lung tissue were clearly higher than those of des-CIC in serum. Clearance appeared to occur in parallel for the lung tissue and the systemic circulation.
Previous studies investigating the distribution of other ICS (fluticasone propionate, beclomethasone dipropionate and budesonide) have used samples from resected pulmonary tissue and confirmed that the experimental approach is appropriate to characterise the pulmonary disposition of ICS 26–29. One study showed high fluticasone propionate concentrations in central lung tissue for a longer time period compared to the tissue concentration in peripheral lung tissue, as well as higher concentrations in the lung tissue than in serum 26. Similarly, concentrations of budesonide in blood plasma were lower than those in lung tissue and concentration levels fall almost in parallel over time 28. Furthermore, following inhalation of beclomethasone dipropionate via a HFA metered-dose inhaler, serum concentrations of beclomethasone-17-monopropionate were lower compared to the lung tissue concentration of this metabolite 27. In a recent study, the deposition of budesonide and fluticasone propionate were directly compared 29. Patients were given single 1,000-μg doses of both budesonide and fluticasone propionate via dry-powder inhalers before lung surgery. In addition to tissue samples from the central and peripheral lung, ex vivo bronchial brush samples were taken during surgery. Interestingly, the highest concentration of fluticasone propionate was detected in bronchial brush samples and detectable levels of this drug for ≤18 h, suggesting the presence of undissolved drug-powder particles in the airway lumen. The mean concentrations of budesonide and fluticasone propionate in the peripheral lung tissue at the interval 1–6 h were 4.3 pmol·g−1 and 18.5 pmol·g−1, respectively 29. Overall, this is a similar order of magnitude compared to des-CIC with a median value of 8.33 pmol·g−1 in the interval of 2–4 h. However, interstudy comparisons should be interpreted with caution, due to variables such as the bioanalytical assays used, the special populations studied, the low number of patients included and the devices used. In the previously mentioned study, the intracellular esterification of budesonide in vivo was confirmed but was not observed for fluticasone propionate 29. This is in line with in vitro investigation, using human precision-cut lung slices, demonstrating that des-CIC and budesonide, in contrast to fluticasone propionate, form fatty acid esters 15. Fatty acid esters of budesonide were formed rapidly after inhalation of the drug and budesonide oleate is the major metabolite in the lung. A similar metabolic pathway was confirmed in humans for intracellularly formed des-CIC in vitro, as well as in this in vivo investigation.
The current study has confirmed rapid activation of ciclesonide in the lung in vivo. For example, at the earliest time-point in peripheral lung tissue, the parent compound ciclesonide represented 21.5% of the total drug concentration (10.9 pmol·g−1), compared with 78.5% (39.75 pmol·g−1) for the metabolites. In vitro investigation using precision-cut human lung slices has demonstrated that ciclesonide is initially converted to des-CIC and subsequently conjugated with fatty acids, with des-CIC oleate as the main metabolite 14, 15. Using 14C-ciclesonide in vitro and detecting radioactive ciclesonide and metabolites, a complete picture of metabolism can be obtained 14. For all metabolites, reference compounds and sensitive bioanalytical assays are available that were used as the basis for the current study to investigate in vivo metabolism without using radiolabelled drug. It should also be noted that the LLOQ for des-CIC oleate was surprisingly low (0.136 pmol·g−1 based on tissue samples of 0.5 g) and, therefore, was detectable even in very small quantities.
Due to the special patient population in the current study (i.e. patients undergoing elective surgery), a similar study for steady state conditions is not feasible. However, studies in rats following repeated inhalation of ciclesonide for 4 weeks have clearly demonstrated that the active metabolite, as well as the fatty acid ester conjugate, were formed and still detected 27 h following the last inhalation 13.
In conclusion, ciclesonide is rapidly converted to the active metabolite, des-CIC, in central and peripheral human lung tissue in vivo, and des-CIC forms conjugates with fatty acids, in particular oleic acid. The formation and the depot-like storage of reversibly formed des-CIC fatty acid conjugates ≤24 h after inhalation may support the once-daily dosing regimen of ciclesonide.
Acknowledgments
The authors would like to thank A. Drollmann (formerly an employee of Nycomed GmbH, Kostanz, Germany) for helpful suggestions for the preparation of the study protocol, H.J. Mascher (pharm-analyt Labor GmbH, Baden, Austria) and R. Herzog (Dept of Bioanalytics, Nycomed GmbH) for bioanalytics of the tissue and serum samples. The authors also thank G. Lahu (Dept of Pharmacometrics, Nycomed GmbH) for helpful suggestions during the preparation of this article.
Footnotes
Statement of interest
Statements of interest for R. Nave, H. Boss and H. Magnussen can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received October 30, 2009.
- Accepted February 19, 2010.
- ©ERS 2010
REFERENCES










