


Abstract
Topotecan is primarily eliminated by the kidneys, with 60 to 70% of the dose recovered as topotecan total in the urine. To elucidate the mechanisms of topotecan renal clearance, we evaluated the effect of probenecid on topotecan renal and systemic disposition in mice. Topotecan lactone or hydroxy acid (1.25 mg/kg i.v.) was administered alone or in combination with probenecid (600 or 1200 mg/kg) given by oral gavage 30 min before and 3 hr after topotecan. Serial blood samples (three mice per time point) and urine samples (five mice per treatment arm) were collected during a 6-hr period. Compared with topotecan alone, coadministration of topotecan lactone or hydroxy acid with probenecid (600 mg/kg) decreased topotecan lactone, total, and hydroxy acid systemic clearance, and total renal clearance. The predominant effect of probenecid was to increase hydroxy acid area under the plasma concentration time curve after administration of topotecan lactone (238.8 vs. 109.9 ng·hr/ml alone, P < .05), or hydroxy acid (1297.2 vs. 355.0 ng·hr/ml alone, P < .05). By inhibiting renal tubular secretion, probenecid decreased renal and systemic clearance which led to an increase in topotecan systemic exposure. These data suggest that probenecid primarily inhibited secretion of the anionic hydroxy acid form, and by direct or indirect mechanisms increased topotecan lactone systemic exposure. Topotecan elimination through renal tubular secretion may have clinical relevance for the use of topotecan in patients with altered renal function.
Topotecan, a camptothecin analog, has a wide range of antitumor activity against adult and pediatric malignancies (Creemers et al., 1994;Stewart et al., 1996). The camptothecin analogs exert their pharmacologic activity by interacting with topoisomerase I-DNA complex and prevent resealing of topoisomerase I-mediated single-strand breaks. This ultimately leads to double-strand DNA breaks and apoptosis or cell death (Potmesil, 1994; Gupta et al., 1995; Wall and Wani, 1977). As depicted in figure 1, topotecan has a lactone moiety in the E-ring and undergoes reversible pH-dependent hydrolysis between the lactone (active) and hydroxy acid (inactive) forms (Tanizawa et al., 1994; Pommier et al., 1994). At physiologic pH, in vitro studies of nonprotein containing buffer solutions report approximately 30 to 40% of topotecan in the lactone form (Beijnen et al., 1990), whereas clinical studies have reported values from 17 to 70% in patient plasma samples (Zamboni et al., 1996a; Stewartet al., 1994; Furman et al., 1996). Thus, changes in plasma pH, serum albumin concentration and route of administration may affect the percentage of topotecan in the lactone form (Stewartet al., 1996).
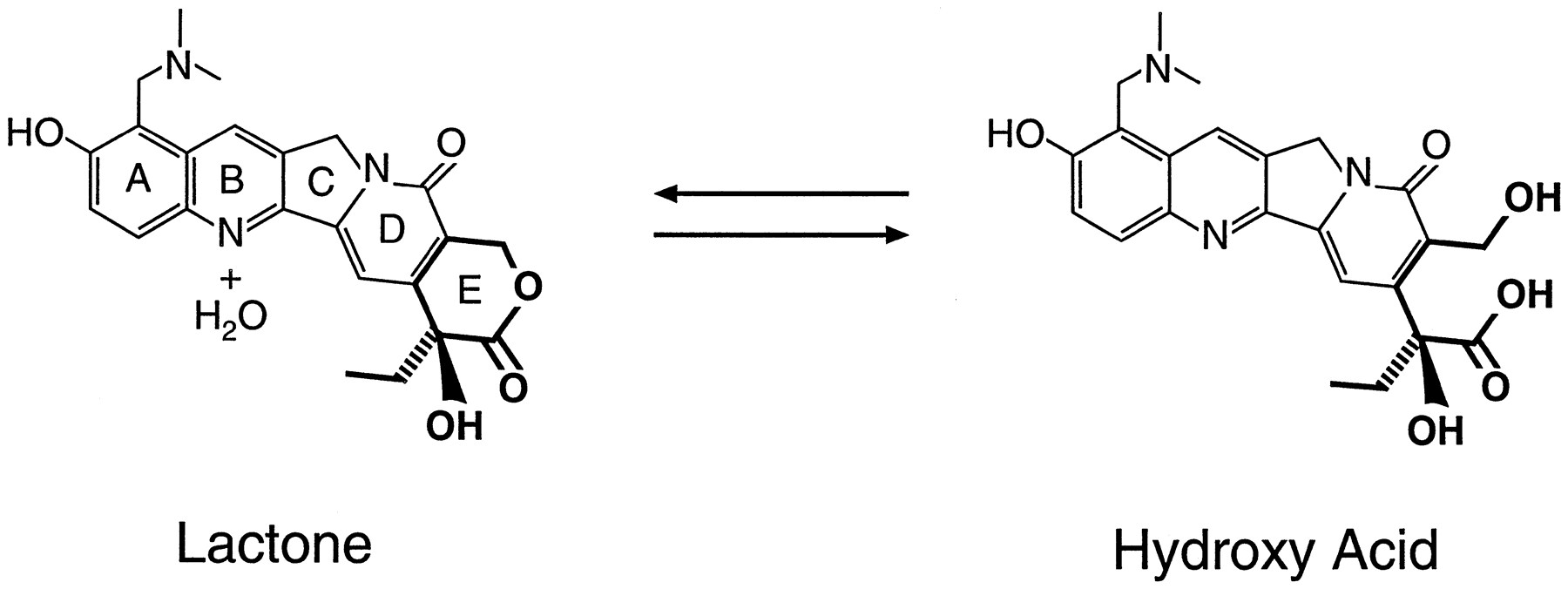
Structure of topotecan lactone and the hydroxy acid form.
Topotecan undergoes both renal and hepatic elimination (Stewartet al., 1994; Furman et al., 1996). In a study of topotecan in adults with liver dysfunction (serum total bilirubin, 1.2–14.9 mg/dL), topotecan disposition was not altered (O’Reillyet al., 1996a). Thus, the authors recommended no topotecan dose modifications in patients with liver dysfunction. In children, topotecan total (sum of topotecan lactone and hydroxy acid) urinary recovery ranges from 60 to 70% (Stewart et al., 1994;Furman et al., 1996). These data suggest that renal clearance is a primary elimination pathway for topotecan. A recent study of topotecan disposition in adults with normal (creatinine clearance (CrCL), 64–171 ml/min) and altered (CrCL, 18–59 ml/min) renal function, reported decreased topotecan renal clearance in patients with renal dysfuction. The authors recommend topotecan dose reductions for patients with creatinine clearance less than 39 ml/min (Slichenmyer et al., 1995). In contrast, we have reported normal topotecan renal and systemic clearance in a patient with a GFR of 19 ml/min/m2 (Zamboni et al., 1996b). Our data suggest that GFR may not be limiting for topotecan clearance, and in patients with decreased GFR, topotecan dose may not need to be reduced because of compensatory clearance by other processes. In addition, topotecan renal and systemic clearance exceeded GFR, which suggests that topotecan is eliminated from the body by renal processes other than GFR, including tubular secretion.
To elucidate the mechanisms of topotecan renal clearance, we studied the ability of probenecid to alter topotecan renal and systemic disposition in mice. Probenecid, an inhibitor of anionic tubular transport in the kidney, alters disposition of organic acids by competitively blocking secretion in the proximal tubule (Cunninghamet al., 1981). The objectives of our study were to evaluate topotecan systemic and renal disposition after administration of the lactone form alone and in combination with probenecid. We also determined the relationship between probenecid dose and schedule and the alteration of topotecan disposition. In addition, because probenecid predominantly inhibits renal tubular secretion of organic acids, we evaluated topotecan disposition after coadministration of anionic-hydroxy acid form alone and with probenecid.
Materials and Methods
Drug formulation and administration.
Topotecan lactone and hydroxy acid were provided by SmithKline Beecham, King of Prussia, PA. Topotecan lactone (0.25 mg/ml) and hydroxy acid (0.25 mg/ml) were dissolved in 0.9% sodium chloride, USP. Topotecan lactone or hydroxy acid (1.25 mg/kg; 4.2 mg/m2) was administered to mice (female CBA/CaJ mice, 30–35 g, 4–6 months of age, Jackson Laboratories, Bar Harbor, ME) by direct injection (duration of infusion <1 min) into a lateral tail vein, alone or in combination with oral probenecid. Probenecid suspension (120 mg/ml) was prepared by triturating commercially available tablets (Schein Pharmaceutical, Florham Park, NJ) and adding the appropriate volume of sterile water, USP (SoloPak Labs. Inc., Elk Grove Village, IL). Probenecid was administered by oral gavage at doses of 300 and 600 mg/kg 30 min before administration of topotecan, and at 600 and 1200 mg/kg 30 min before and 3 hr after administration of topotecan.
Sample collection and analysis.
Topotecan pharmacokinetic values were evaluated in mice after a single dose of topotecan lactone or hydroxy acid alone and in combination with probenecid. All procedures were approved by our Animal Resources Committee. Heparinized blood samples (approximately 1 ml) were collected (three mice per time point by cardiac puncture after methoxyflurane anesthesia) before, 0.25, 1, 2, 4 and 6 hr after administration. All plasma samples were handled and processed as previously described in detail (Stewartet al., 1994). To reliably quantitate topotecan lactone and to prevent conversion between the lactone and hydroxy acid forms during sample processing, plasma was separated from whole blood immediately, and 200 μl of plasma was placed in 800 μl of cold (−30°C) methanol within 3 min of obtaining the sample (Stewart et al., 1994). The mixture was vortexed for 10 sec, centrifuged for 2 min at 12,000 rpm in a rapid table-top centrifuge, and the supernatant was decanted into a plastic screw-top tube. A separate 400-μl sample of plasma methanol extract was acidified with 20 μl of 20% phosphoric acid for analysis of topotecan total (lactone plus hydroxy acid). Topotecan hydroxy acid plasma concentrations were calculated as the difference between total and lactone concentrations.
In a separate experiment, urine samples were collected from individual mice (n = 5 per treatment arm) during a 6-hr period after administration of 1.25 mg/kg i.v. of topotecan lactone or hydroxy acid alone and in combination with oral probenecid (600 and 1200 mg/kg) 30 min before and 3 hr after topotecan. To obtain sufficient urine volume for analysis, 5% dextrose in water (USP), 0.6 μl/min, was infused into a lateral tail vein during the 6-hr collection period. Methoxyflurane anesthesia was used before placement of the catheter into the lateral tail vein. Conscious mice were then placed into individual restraint compartments, and urine was collected in containers placed under the restraint compartments. At the end of the 6-hr collection period, mice were sacrificed by cervical dislocation.
Urine samples were prepared by adding 200 μl of sample to 800 μl of cold (−30°C) methanol, vortexed and centrifuged as described above. A 400-μl aliquot of urine methanol extract was acidified with 20 μl of 20% phosphoric acid for analysis of topotecan total (lactone plus hydroxy acid) (Beijnen et al., 1990; Stewart et al., 1994). Topotecan total was quantitated in the urine, as the concentration of topotecan lactone and hydroxy acid vary with pH, and changes in urine pH (5 to 8) may produce widely divergent individual values.
Topotecan high-performance liquid chromatography.
A sensitive and specific isocratic high-performance liquid chromatography assay with fluorescence detection (Shimadzu RF535, Columbia, MD) was used to determine topotecan lactone and total plasma concentrations, and total urine concentrations (Baker et al., 1996; Tubergenet al., 1996; Stewart et al., 1994; Beijnenet al., 1990). Topotecan was detected by a fluorescence detector with excitation at 380 nm and emission at 520 nm. Retention times and peak heights were calculated by a data integration system (Shimadzu CR501, Columbia, MD). Calibration curves were constructed with use of spiked pooled murine plasma and urine (Hilltop Animal Laboratories, Scottsdale, PA), with ranges of 0.25 to 300 ng/ml and 5 to 70 μg/ml, respectively. The lower limit of sensitivity for the assay was 0.25 ng/ml.
Pharmacokinetic analysis.
A two-compartment model with maximum likelihood estimation was fit to topotecan lactone and total plasma concentration data after administration of lactone, and topotecan hydroxy acid and total plasma concentration data after administration of hydroxy acid (ADAPT II) (D’Argenio and Schumitzky, 1990). Model parameters estimated included the volume of the central compartment (Vc), elimination rate constant (ke) and the intercompartment rate constants (kcp,kpc). With standard equations, systemic clearance (Clsys) and volume of distribution at steady state (Vdss) were calculated from parameter estimates (Gibaldi and Perrier, 1982). Area under the plasma concentration-time curve from zero to infinity (AUC0→ ∞) and from 0 to 6 hr (AUC0–6 hr) were calculated by the log-linear trapezoidal method (Yeh and Kwan, 1978). Topotecan total renal clearance (Clrenal) was calculated by dividing the amount of topotecan total recovered in the urine from 0 to 6 hr by the topotecan total plasma AUC0–6 hr. Topotecan hydroxy acid and lactone plasma concentration data after topotecan lactone and hydroxy acid administration, respectively, were analyzed by noncompartmental methods (Gibaldi and Perrier, 1982).
Statistical analysis.
Compartmental pharmacokinetic parameters describing systemic disposition were determined from the average concentration of three mice at each time point. Thus, pharmacokinetic parameters describing topotecan systemic disposition are reflected as a single value. The concentration-time profile was modeled through a gamma shape curve, and model parameters were examined by applying linear regression to log concentration. The interaction among time, log time and treatment effect was evaluated byF-test in the linear regression (Neter et al., 1990). R2 was used to examine the model fitness.
In contrast to pharmacokinetic parameters describing topotecan systemic disposition, the effect of probenecid on topotecan renal clearance was performed with each mouse representing an individual result. Thus, differences between renal clearance rates were compared by the Kruskal-Wallis test (Lehmann, 1975), multiple comparisons were adjusted by Duncan’s procedures (Hochberg and Tamhane, 1987), and data are presented as mean ± standard deviation.
Results
Effect of probenecid dose and schedule on topotecan disposition.
Administration of 300 mg/kg probenecid as a single dose 30 min before topotecan lactone did not change topotecan systemic disposition (data not shown). Probenecid (600 mg/kg) on the same schedule did alter topotecan systemic disposition for up to 4 hr after administration of topotecan, but from 4 to 6 hr the effect was not maintained (data not shown). However, the alteration of topotecan systemic disposition was maintained for the entire 6-hr study period with two doses of probenecid, 600 and 1200 mg/kg (i.e., 30 min before and 3 hr after administration of topotecan). Thus, we performed all further evaluations of topotecan systemic and renal disposition with the two-dose schedule of probenecid administration.
Effect of probenecid on topotecan systemic disposition after administration of topotecan lactone.
Topotecan lactone, hydroxy acid and total plasma concentration time plots after administration of topotecan lactone alone and in combination with probenecid are presented in figure 2. Topotecan pharmacokinetic parameters after administration of topotecan lactone are summarized in table 1. Topotecan lactone and total systemic clearance were less after coadministration of probenecid (600 or 1200 mg/kg) compared with their disposition after topotecan alone. As shown in table 2, when topotecan lactone is given with probenecid (600 or 1200 mg/kg) the lactone, hydroxy acid and total systemic exposure are greater than in the absence of probenecid (P < .05). Further analysis shows the increase in hydroxy acid systemic exposure is greater than the increase in lactone systemic exposure at either dose of probenecid.

Topotecan lactone (a), total (b) and hydroxy acid (c) plasma concentration-time profile after administration of topotecan lactone alone and in combination with probenecid. Individual data points and best-fit line of the data are represented for topotecan lactone alone (—, •), and in combination with probenecid 600 mg/kg (– –, □), and 1200 mg/kg (- - -, ▵).
Topotecan pharmacokinetic parameters after administration of topotecan lactone
Topotecan systemic exposures after administration of topotecan lactone and hydroxy acid
Effect of probenecid on topotecan systemic disposition after administration of topotecan hydroxy acid.
Our results demonstrating that probenecid predominately alters topotecan hydroxy acid disposition led us to evaluate the effect of probenecid on topotecan disposition after administration of the hydroxy acid form. Topotecan lactone, hydroxy acid and total plasma concentration profiles after administration of topotecan hydroxy acid alone and in combination with probenecid are presented in figure3. Because the 600 and 1200 mg/kg probenecid dose produced similar results in the previous experiments, we chose to use the 600 mg/kg probenecid dose for subsequent experiments. Topotecan pharmacokinetic parameters after administration of topotecan hydroxy acid are presented in table3. Coadministration of 600 mg/kg probenecid with topotecan hydroxy acid resulted in a similar decrease in topotecan hydroxy acid and total systemic clearances (∼3-fold). As shown in table 2, administration of probenecid with topotecan hydroxy acid resulted in greater increases in the topotecan lactone, total and hydroxy acid systemic exposures than with the administration of topotecan hydroxy acid alone (P < .05).

Topotecan lactone (a), total (b) and hydroxy acid (c) plasma concentration-time profile after administration of topotecan hydroxy acid alone and in combination with probenecid. Individual data points and best-fit line of the data are represented for topotecan hydroxy acid alone (—, •) and in combination with 600 mg/kg probenecid (– –, □).
Topotecan pharmacokinetic parameters after administration of topotecan hydroxy acid
Effect of probenecid on topotecan renal disposition after administration of topotecan lactone or hydroxy acid.
Topotecan total renal clearance is summarized in table 1. The combination of topotecan lactone and probenecid (600 or 1200 mg/kg) resulted in 44% and 30% decrease in topotecan total renal clearance compared with topotecan alone, respectively (P < .05). Moreover, the administration of topotecan hydroxy acid and probenecid resulted in a 71% decrease in topotecan total renal clearance (table 3 and fig.4) (P < .05).

Topotecan total renal clearance (Clr) after administration of topotecan lactone and hydroxy acid alone and in combination with probenecid (600 and 1200 mg/kg). The box defines the mean ± one standard deviation. The mean is depicted as the horizontal line within each box. Lines extending from the top and bottom of each box denote range (maximum and minimum) of observed values. Coadministration of probenecid (600 and 1200 mg/kg) with topotecan lactone and probenecid (600 mg/kg) with topotecan hydroxy acid significantly reduced topotecan Clr as compared with topotecan alone (P < .05).
Discussion
Although we and other investigators have reported topotecan systemic and renal disposition in humans (O’Reilly et al., 1996b; Slichenmyer et al., 1994; Stewart et al., 1994; Furman et al., 1996), we provide the first data showing that topotecan undergoes anionic renal tubular secretion. The potential clinical importance of these data are underscored by the increase in systemic exposure of the active-lactone form of topotecan when administered concomitantly with other agents which undergo anionic renal tubular secretion, such as probenecid, indomethacin, penicillin and methotrexate (Cunningham et al., 1981; Weiner, 1979;Poulsen, 1955). Coadministration of these agents with topotecan may result in an increase in lactone systemic exposure, with a subsequent increase in toxicity and or antitumor effect. The addition of renal tubular secretion to glomerular filtration as a mechanism of topotecan renal clearance provides a basis for our previously reported observation of unimpaired renal clearance in a patient with decreased glomerular filtration (Zamboni et al., 1996b). Thus, based on the data of the present study we propose that topotecan dosage reductions may not be necessary in patients with decreased glomerular filtration because of clearance by other pathways, including renal tubular secretion.
After administration of topotecan lactone or hydroxy acid, data suggest that probenecid inhibits topotecan renal tubular secretion, which results in a decrease in topotecan renal and systemic clearance and subsequent increase in topotecan lactone, hydroxy acid and total systemic exposure. The greatest increase in systemic exposure occurred with the hydroxy acid, which suggests that coadministration of probenecid predominantly inhibits the secretion of this anionic form. Consistent with probenecid primarily affecting the anionic form, coadministration of probenecid with topotecan hydroxy acid resulted in 2.6-fold higher percent increase in hydroxy acid AUC compared with lactone AUC. The almost identical percent decrease in hydroxy acid and total systemic clearance (i.e., 68% and 66%, respectively) after coadministration of topotecan hydroxy acid and probenecid, provides further evidence which suggests that probenecid predominantly affects the hydroxy acid form.
Comparison of probenecid effects after administration of topotecan lactone and hydroxy acid further suggest probenecid predominantly inhibits renal tubular secretion of the hydroxy acid form. Coadministration of probenecid with topotecan hydroxy acid resulted in a greater decrease in topotecan total systemic clearance and renal clearance than lactone administration. The combination of probenecid resulted in a 2.7-fold increase in topotecan total systemic exposure after administration of hydroxy acid than lactone administration. In addition, after administration of topotecan lactone and hydroxy acid the percent increases in hydroxy acid systemic exposure were 3.3- and 2.6-fold higher than the increase in lactone systemic exposure.
After administration of topotecan lactone or hydroxy acid, a pH-dependent reversible conversion occurs between the lactone and hydroxy acid forms (fig. 1). Our data suggest that probenecid predominantly inhibits the renal tubular secretion of the hydroxy acid form, thus the increase in the active-lactone systemic exposure after administration of topotecan lactone or hydroxy acid results from two possible mechanisms. Probenecid may directly block lactone renal tubular secretion, but to a lesser degree than hydroxy acid, thus increasing lactone systemic exposure. Alternatively, probenecid may indirectly increase topotecan lactone systemic exposure by inhibiting hydroxy acid tubular secretion. The increase in hydroxy acid systemic exposure may then shift the hydrolysis equilibrium toward systemic formation of the lactone form.
Probenecid is a competitive blocker of anionic renal tubular secretion (Cunningham et al., 1981). Prior studies in rodents have administered probenecid by intravenous or intraperitoneal routes (Aibaet al., 1994; Sandstrom, 1986; Tsuji et al., 1983; Klecker et al., 1994; Ban et al., 1994). However, we were unable to obtain or formulate a probenecid solution suitable for intravenous or intraperitoneal administration, and thus had to use oral administration of a probenecid suspension. The optimal dose of probenecid which inhibits anionic tubular secretion in mice has not been determined (Sandstrom, 1986; Tsuji et al., 1983;Klecker et al., 1994; Ban et al., 1994). Therefore, oral probenecid was administered either once or twice daily, and the dose escalated to determine the schedule of probenecid which had the greatest effect on topotecan systemic and renal disposition. Coadministration of 300 mg/kg probenecid did not significantly alter topotecan systemic disposition, whereas probenecid (600 and 1200 mg/kg) produced similar effects. Thus, the probenecid dose which achieves maximum inhibition of topotecan renal tubular secretion is greater than 300 mg/kg and less than or equal to 600 mg/kg when given before and 3 hr after topotecan administration. The decrease in topotecan systemic clearance noted after administration of probenecid was greater than the decrease in renal clearance, which suggests that probenecid may also inhibit other excretory pathways (e.g., biliary secretion) (Wall et al., 1992). Urinary creatinine excretion was not monitored as an independent measure of renal function.
Use of preclinical animal models to describe and evaluate the pharmacokinetic disposition of drugs for human use requires similar pharmacokinetic handling of the drug by the animal model and humans. Mice have renal physiology similar to primates, including humans (Kaplan et al., 1983). Also, mice have been widely used as preclinical models to evaluate potentially toxic renal agents, and mechanisms of renal drug elimination (Sandstrom, 1986; Kutteschet al., 1982; Nightingale et al., 1975). Topotecan systemic disposition in mice (Houghton et al., 1992) is similar to topotecan systemic disposition in humans (O’Reillyet al., 1996b; Slichenmyer et al., 1994; Stewartet al., 1994; Furman et al., 1996). However, topotecan total renal clearance in humans was approximately 48% of total systemic clearance (Zamboni et al., 1996b) compared with 2.5% in mice after administration of topotecan lactone. This suggests that probenecid alters topotecan systemic disposition by inhibiting topotecan elimination by a second process in addition to renal tubular secretion, possibly biliary tubular secretion. In addition, the lower renal clearance of topotecan total after hydroxy acid alone compared with lactone administration alone suggest that the anionic-hydroxy acid form undergoes elimination by a process in addition to renal tubular secretion. Regardless of the primary clearance pathway of topotecan in mice, the clinical significance of this drug interaction is underscored the by ability of probenecid to inhibit topotecan renal and systemic clearance, the 3-fold higher topotecan renal clearance compared with glomerular filtration in humans (Zamboni et al., 1996b), and the steep relationship between topotecan exposure and response (i.e., toxicity or antitumor) (Zamboni et al., 1996a; Stewart et al., 1994; Furman et al., 1996). Thus, agents such as probenecid, which inhibit anionic renal tubular secretion, may have an even greater effect in humans than in mice.
In conclusion, by inhibiting renal tubular secretion, probenecid has been shown to decrease topotecan renal and systemic clearance and increase topotecan systemic exposure after administration of lactone or hydroxy acid. In addition, these data suggest that probenecid predominantly inhibits secretion of the anionic hydroxy acid form. Probenecid also increases the systemic exposure of the active lactone form, either by directly inhibiting lactone renal tubular secretion or indirectly by inhibiting hydroxy acid secretion with subsequent systemic conversion to the lactone form. Topotecan undergoing renal tubular secretion has clinically significant ramifications and requires further in vitro and in vivo studies to determine the exact mechanisms by which inhibition of anionic renal tubular secretion increases the active lactone form of topotecan.
Footnotes
-
Send reprint requests to: Clinton F. Stewart, Pharm.D., Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, 332 N. Lauderdale, Memphis, TN 38105.
-
↵1 This work was supported in part by US Public Health Service award CA23099, Cancer Center Support grant CA21765 and by American, Lebanese, Syrian Associated Charities (ALSAC).
- Abbreviations:
- AUC
- area under the plasma concentration time curve
- GFR
- glomerular filtration rate
- Received April 11, 1997.
- Accepted September 15, 1997.
- The American Society for Pharmacology and Experimental Therapeutics




{kind=link}
{kind=link}
{kind=link}
{kind=link}