


Abstract
The cardioprotective efficacy of zoniporide (CP-597,396), a novel, potent, and selective inhibitor of the sodium-hydrogen exchanger isoform 1 (NHE-1), was evaluated both in vitro and in vivo using rabbit models of myocardial ischemia-reperfusion injury. In these models, myocardial injury was elicited with 30 min of regional ischemia and 120 min of reperfusion. Zoniporide elicited a concentration-dependent reduction in infarct size (EC50 of 0.25 nM) in the isolated heart (Langendorff) and reduced infarct size by 83% (50 nM). This compound was 2.5- to 20-fold more potent than either eniporide or cariporide (EC50 of 0.69 and 5.11 nM, respectively), and reduced infarct size to a greater extent than eniporide (58% reduction in infarct size). In open-chest, anesthetized rabbits, zoniporide also elicited a dose-dependent reduction in infarct size (ED50of 0.45 mg/kg/h) and inhibited NHE-1-mediated platelet swelling (maximum inhibition 93%). Furthermore, zoniporide did not cause any in vivo hemodynamic (mean arterial pressure, heart rate, rate pressure product) changes. Zoniporide represents a novel class of potent NHE-1 inhibitors with potential utility for providing clinical cardioprotection.
The sodium-hydrogen exchanger (NHE) is a key component of the heart's response to intracellular acidosis following an ischemic insult. Presently, there are at least six known NHE isoforms (NHE-1–6), although NHE-1 (which is ubiquitously expressed) is by far the predominant cardiac isoform (Orlowski et al., 1992; Noel and Pouyssegur, 1995; Yun et al., 1995;Orlowski and Grinstein, 1997). Upon reperfusion of the ischemic myocardium, NHE-1 activation leads to a rise in [Na+]i (Xiao and Allen, 1999), followed by a subsequent increase in [Ca2+]i as Na+ is pumped out of the cardiomyocyte by the sodium-calcium exchanger; this accumulation of intracellular Ca2+ contributes to the activation of various proteases, cardiomyocyte contracture, arrhythmias, and cell death (for recent reviews, see Scholz and Albus, 1995; Frohlich and Karmazyn, 1997; Karmazyn et al., 1999).
Since NHE-1 activation during reperfusion is clearly detrimental to the heart, inhibition of this exchanger before reperfusion should reduce the associated myocardial damage. The first confirmation of this hypothesis was provided by Karmazyn (1988) who showed that amiloride enhanced ventricular recovery and diminished enzyme efflux from isolated rat hearts subjected to ischemia/reperfusion. Numerous studies have since confirmed these observations (Scholz and Albus, 1995;Frohlich and Karmazyn, 1997; Karmazyn et al., 1999), and more recently, NHE-1 inhibitors of either greater potency and/or selectivity (e.g., cariporide/HOE 642, EMD 85131, BIIB 513) than amiloride have been demonstrated to be cardioprotective in animal models (Scholz et al., 1995; Gumina et al., 1998, 1999; Aye et al., 1999; Humphreys et al., 1999; Spitznagel et al., 2000) and in humans (Rupprecht et al., 2000).
Given the potential clinical benefit of NHE-1 inhibition during myocardial ischemia/reperfusion, zoniporide {CP-597,396; [1-(quinolin-5-yl)-5-cyclopropyl-1H-pyrazole-4-carbonyl]guanidine hydrochloride monohydrate} was identified and characterized (Guzman-Perez et al., 2001; R. B. Marala, J. A. Brown, J. X. Kong, W. R. Tracey, D. R. Knight, R. T. Wester, D. Sun, S. P. Kennedy, E. S. Hamanaka, R. B. Ruggeri, and R. J. Hill, submitted). This compound is a novel, potent, and highly selective human NHE-1 inhibitor (200- and >800-fold versus NHE-2 and NHE-3, respectively), which inhibits NHE-1-dependent22Na+ uptake with an IC50 of 14 nM (R. B. Marala, J. A. Brown, J. X. Kong, W. R. Tracey, D. R. Knight, R. T. Wester, D. Sun, S. P. Kennedy, E. S. Hamanaka, R. B. Ruggeri, and R. J. Hill, submitted). In this report, we describe the cardioprotective efficacy of zoniporide in both in vitro and in vivo rabbit models of myocardial ischemic injury, and compare the efficacy of zoniporide to cariporide and eniporide, two other NHE-1 inhibitors currently in clinical trials.
Materials and Methods
This investigation conforms to the Guide for the Care and Use of Laboratory Animals published by the Institute of Laboratory Animal Resources (National Research Council, 1996).
In Vitro (Langendorff) Preparation.
Male New Zealand White rabbits (3–4 kg; Covance, Denver, PA) were anesthetized by i.v. administration of sodium pentobarbital (30 mg/kg), followed by intubation and ventilation with 100% O2 using a positive pressure ventilator. A left thoracotomy was performed, the heart exposed, and a snare (2-0 silk) placed loosely around a prominent branch of the left coronary artery. The heart was rapidly removed from the chest, mounted on a Langendorff apparatus, and maintained by retrograde perfusion (nonrecirculating) with a modified Krebs' solution (118.5 mM NaCl, 4.7 mM KCl, 1.2 mM MgSO4, 1.2 mM KH2PO4, 24.8 mM NaHCO3, 2.5 mM CaCl2, and 10 mM glucose) at a constant pressure of 80 mm Hg and a temperature of 38.5°C. Perfusate pH was maintained at 7.4 to 7.5 by bubbling with 95% O2, 5% CO2. The temperature of the heart was maintained by suspending it in a heated, water-jacketed organ bath. A fluid-filled latex balloon was inserted in the left ventricle and connected by stainless steel tubing to a pressure transducer; the balloon was inflated to provide a systolic pressure of 80 to 120 mm Hg, and a diastolic pressure ≤10 mm Hg. Heart rate (HR), left ventricular systolic and diastolic pressures, and left ventricular developed pressure (LVDP) were recorded using a PO-NE-MAH Data Acquisition and Archive System (Gould Instrument Systems, Valley View, OH). Total coronary flow rate (CF) was determined using an in-line flow probe (Transonic Systems, Inc., Ithaca, NY); CF was normalized for heart weight. Each heart was allowed to equilibrate for 30 min; if stable left ventricular pressures within the parameters outlined above were not observed, the heart was discarded. Pacing was not used unless the heart rate fell below 180 bpm before the 30-min period of regional ischemia; in this case, the heart was paced at 200 bpm, which was the average spontaneous rate observed.
Langendorff Experimental Protocols.
Zoniporide, cariporide, or eniporide perfusion was begun 30 min before regional ischemia and was continued for the duration of the experiment (Fig.1). Thirty minutes of regional ischemia was produced by tightening the snare around the branch of the coronary artery. At the end of this period, the snare was released and the heart reperfused for an additional 120 min. Control hearts did not receive any drug.

Experimental protocols.
In Vivo Preparation.
Thirty-seven fed New Zealand White male rabbits (3–4 kg) were anesthetized with sodium pentobarbital (30 mg/kg i.v.) and a surgical plane of anesthesia was maintained by a continuous infusion of sodium pentobarbital (16 mg/kg/h) via an ear vein catheter. A tracheotomy was performed through a ventral midline cervical incision and the rabbits were ventilated with 100% oxygen using a positive pressure ventilator. Body temperature was maintained at 38.5°C using a heating pad connected to a YSI temperature controller model 72 (Yellow Springs Instruments, Yellow Springs, MD). Fluid-filled catheters were placed in the left jugular vein for drug administration and in the left carotid artery for blood pressure measurements and for blood gas analysis using a model 248 blood gas analyzer (Bayer Diagnostics, Norwood, MA). The ventilator was adjusted as needed to maintain blood pH and pCO2 within normal physiological ranges for rabbits. The heart was exposed through a left thoracotomy at the 4th intercostal space and a 2-0 silk suture was placed around a prominent branch of the left coronary artery. Lead II ECG was measured using an ECG amplifier (Gould Inc., Cleveland, OH) connected to surface ECG electrodes. Arterial pressure was measured using a calibrated strain gauge transducer (Spectromed, Oxnard, CA) connected to the arterial catheter. HR and mean arterial pressure (MAP) were derived using the PO-NE-MAH Data Acquisition and Archive System. Rate pressure product (RPP) was calculated as the product of HR and MAP. RPP has been previously used as an index of myocardial O2 consumption in this model (Kingma et al., 1994).
In Vivo Experimental Protocols.
Ninety minutes after surgery, when arterial pressure, HR, and RPP had stabilized for at least 30 min (baseline) the experiment was started following the protocol shown in Fig. 1. Zoniporide or vehicle infusion was begun 30 min before regional ischemia and continued for a total of 2 h. Regional ischemia was produced by tightening the coronary artery snare for 30 min. The snare was released, and the heart was reperfused for an additional 120 min. Myocardial ischemia was evidenced by regional cyanosis and ST segment elevation; reperfusion was confirmed by reactive hyperemia and rapid decline of the ST elevation. At the end of reperfusion, each rabbit was euthanized with an intravenous overdose of sodium pentobarbital (100 mg/kg). The heart was quickly excised, mounted on a Langendorff apparatus, and perfused with physiological saline at 38.5°C.
Determination of Infarct Size.
After completion of each experiment (in vitro or in vivo) and with the heart suspended and perfused on the Langendorff apparatus, the coronary artery snare was retightened, and a 0.5% suspension of fluorescent zinc cadmium sulfate particles (1–10 μm) was perfused through the heart to delineate the area-at-risk (nonlabeled) in the left ventricle (LV) for infarct development. The heart was removed from the Langendorff apparatus, blotted dry, weighed, wrapped in aluminum foil, and stored overnight at −20°C. Frozen hearts were sliced into 2-mm transverse sections and incubated with 1% triphenyl tetrazolium chloride in phosphate-buffered saline for 20 min at 37°C to delineate noninfarcted (stained) from infarcted (nonstained) LV tissue. The infarct area and the area-at-risk were calculated for each slice of left ventricle using video-captured images and ETC3000 image analysis software (Engineering Technology Center, Mystic, CT), followed by adding the values for each tissue slice to obtain the total infarct area and total area-at-risk for each heart. To normalize the infarct area for differences in the area-at-risk between hearts, the infarct size was expressed as the ratio of infarct area versus area-at-risk (% IA/AAR).
Platelet Swelling Assay.
The effect of NHE-1 inhibitors on platelet swelling was performed as described by Rosskopf et al. (1991), with minor modifications. Briefly, blood (5–10 ml) was withdrawn from rabbits by venipuncture into tubes containing EDTA. Platelet-rich plasma (PRP) was obtained by centrifugation of whole blood at 170g for 10 min at room temperature. The upper two-thirds of the plasma was removed and used for assessment of platelet swelling. Propionate medium (400 μl; 140 mM sodium propionate, 20 mM HEPES, 10 mM glucose, 5 mM KCl, 1 mM MgCl2, 1 mM CaCl2, pH 6.7) was placed in plastic disposal cuvettes (1-cm path length) in a spectrophotometer (2401PC; Shimadzu, Baltimore, MD) to which samples of PRP were directly added. Changes in optical density at 680 nm were recorded for 5 min at 6-s intervals. All measurements were performed in triplicate at room temperature, and were completed within 4 h of venipuncture. Rate constants were calculated from slopes generated from the first 42 s as previously described (Rosskopf et al., 1991).
Data Expression and Analysis.
Data are expressed as the mean ± S.E. Between-group comparisons of in vitro and in vivo areas-at-risk expressed as a percentage of left ventricular areas (% AAR/LV) were compared using ANOVA. Comparisons of in vivo hemodynamic parameters between zoniporide and vehicle control over the course of the study were performed using ANOVA with repeated measures. In vitro hemodynamics and platelet swelling comparisons were performed byt test, whereas in vitro and in vivo % IA/AAR values were compared using a Mann-Whitney test; a Bonferroni correction was applied to multiple comparisons. A P value of less than 0.05 was considered statistically significant.
Drugs and Drug Preparation.
Zoniporide (Guzman-Perez et al., 2001), cariporide (HOE 642), and eniporide (EMD 96785) were synthesized at Pfizer Global Research and Development (Groton, CT). All drugs administered to the isolated hearts were dissolved in dimethyl sulfoxide and diluted in buffer; the final dimethyl sulfoxide concentration was less than 0.1%, which had no effect on infarct size (Tracey et al., 1997). For the in vivo studies, zoniporide was dissolved in normal saline, at concentrations ranging from 0.15 to 2.5 mg/ml and was delivered at a constant volume of 5 ml/h over 2 h.
Results
In the Langendorff hearts, LVDP and CF were significantly (P < 0.05) reduced in all groups by occlusion of the coronary artery, confirming that ischemia was achieved in all groups (Table 1). The % AAR/LV was 29 ± 2% (n = 6) for the Langendorff control group; % AAR/LV values for the remaining in vitro groups were not significantly different from the control group.
Hemodynamic data from isolated rabbit hearts
Zoniporide elicited a significant (P < 0.05) concentration-dependent reduction in infarct size in the isolated rabbit hearts (Figs. 2 and3), reducing the % IA/AAR from 53 ± 3% (control) to 9 ± 1% (50 nM zoniporide). Compared with cariporide, zoniporide was approximately 20-fold more potent and produced an equivalent maximum reduction in infarct size, whereas compared with eniporide, zoniporide was approximately 2.5-fold more potent, and produced a greater degree of cardioprotection (Fig. 3; Table 2).

Effect of zoniporide on % IA/AAR in isolated rabbit hearts. Zoniporide was constantly perfused through the hearts beginning 30 min before the regional ischemia, as described underMaterials and Methods. Infarct area and area-at-risk were determined by image analysis and infarct area was normalized for area-at-risk (% IA/AAR). Data are the mean ± S.E. for each group, n = 5 to 12. *Significantly different (P < 0.05) from control.

Comparison of cardioprotection provided by zoniporide, cariporide, and eniporide, in isolated rabbit hearts. Each drug was constantly perfused through the hearts beginning 30 min before the regional ischemia, as described under Materials and Methods. Infarct area and area-at-risk were determined by image analysis and infarct area was normalized for area-at-risk (% IA/AAR). Data are the mean ± S.E. for each group, n = 5 to 12.
Comparison of zoniporide, cariporide, and eniporide
In the in vivo model, the % AAR/LV value for the untreated control group was 36 ± 2% (n = 15); the % AAR/LV values for the remaining in vivo groups were not significantly different (P ≥ 0.05) from the control.
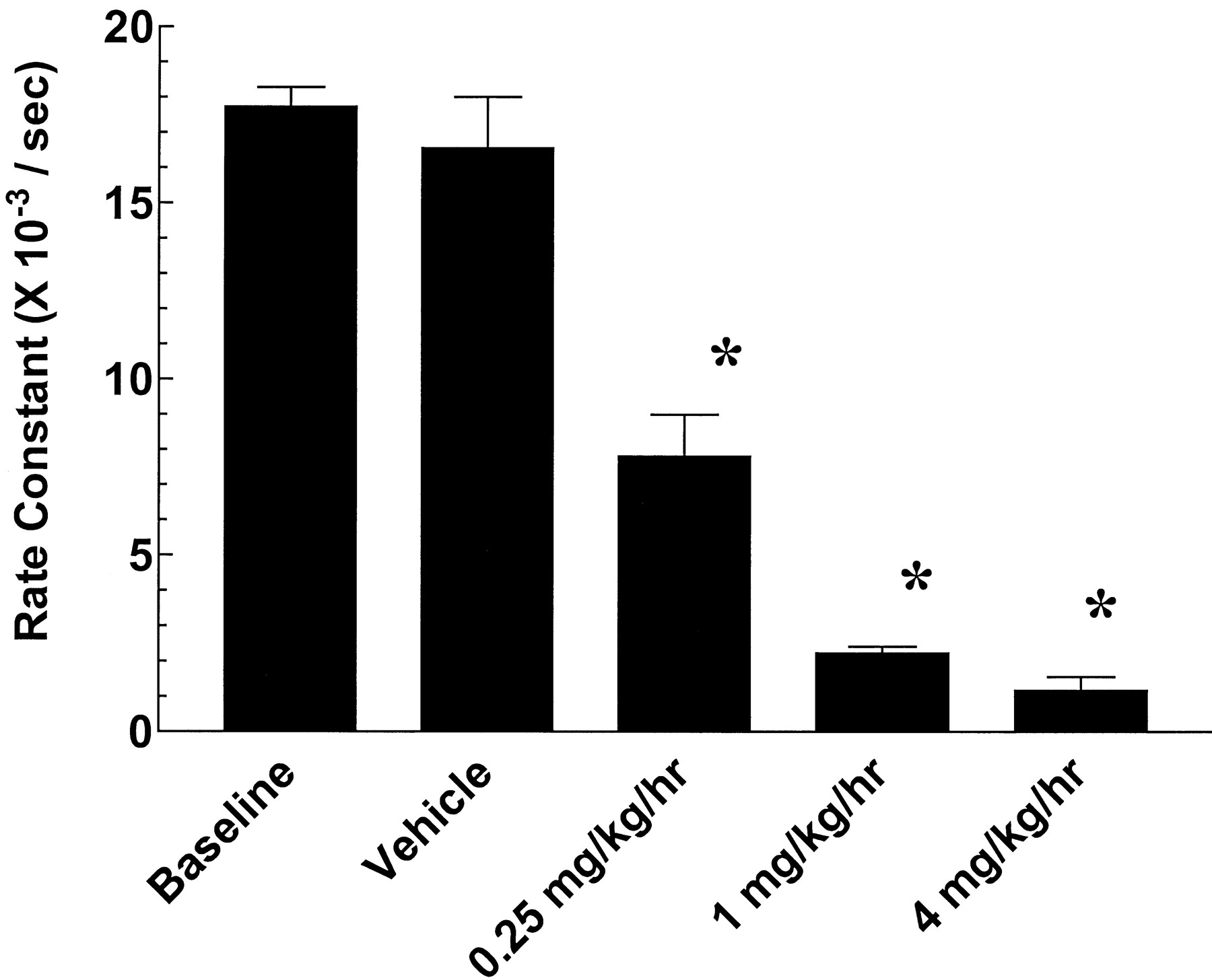
The effects of zoniporide on MAP, HR, and RPP in the anesthetized rabbit are illustrated in Fig. 4; no significant effects of zoniporide on any of these hemodynamic variables were observed when compared with the vehicle control. Zoniporide produced a significant (P < 0.05) dose-dependent reduction in infarct size in the anesthetized rabbit (Fig.5). The % IA/AAR was decreased by 75% at a dose of 4 mg/kg/h, from 57 ± 3% (vehicle control) to 14 ± 2%; the ED50 was 0.45 mg/kg/h. In addition, zoniporide demonstrated a dose-dependent reduction in NHE-1-mediated platelet swelling (ID50 of 0.21 mg/kg/h); a dose of 4 mg/kg/h reduced platelet swelling by 93% (Fig.6).

Effect of zoniporide and vehicle control on HR (A), MAP (B) and RPP (C) in anesthetized rabbits. Zoniporide or vehicle control was infused for 2 h, beginning 30 min before the regional ischemia, as described under Materials and Methods. Zoniporide had no significant effect on these hemodynamic parameters over the course of the study when compared with vehicle control. Data are the mean ± S.E. for each group, n = 6 to 15.

Effect of in vivo administration of zoniporide on % IA/AAR in anesthetized rabbits. Zoniporide or vehicle control was infused for 2 h, beginning 30 min before the regional ischemia, as described under Materials and Methods. Infarct area and area-at-risk were determined by image analysis and infarct area was normalized for area-at-risk (% IA/AAR). Data are the mean ± S.E. for each group, n = 6 to 15. *Significantly different (P < 0.05) from control.

Effect of in vivo administration of zoniporide on NHE-1-mediated platelet swelling. After 1 h of zoniporide infusion, blood samples were withdrawn, and platelet swelling in response to intracellular acidification evaluated, as described underMaterials and Methods. Data are the mean ± S.E. for each group, n = 4. *Significantly different (P < 0.05) from control.
Discussion
The role of Na+/H+exchange in the cardiac response to ischemic injury became evident shortly before the cloning of the first Na+/H+ exchanger over 10 years ago (Sardet et al., 1989), when amiloride was demonstrated to enhance ventricular recovery and reduce myocardial damage in isolated rat hearts subjected to ischemia/reperfusion (Karmazyn, 1988). Since then, at least six different NHE isoforms have been identified, although the predominant cardiac isoform is NHE-1 (Orlowski et al., 1992; Noel and Pouyssegur, 1995; Yun et al., 1995; Orlowski and Grinstein, 1997). Numerous studies have further elucidated the role of NHE-1 in various aspects of cardiac pathophysiology, including myocardial stunning (du Toit and Opie, 1993; Sack et al., 1994; Myers and Karmazyn, 1996; Symons et al., 1998), arrhythmogenesis (Scholz et al., 1993, 1995; Yasutake et al., 1994; Aye et al., 1999; Humphreys et al., 1999), cardiomyocyte apoptosis (Chakrabarti et al., 1997;Humphreys et al., 1999), infarction (Klein et al., 1995; Rohmann et al., 1995; Gumina et al., 1998, 1999; Aye et al., 1999), and hypertrophy (Hasegawa et al., 1995; Spitznagel et al., 2000; Yoshida and Karmazyn, 2000). Importantly, NHE-1 inhibition has been found to reduce the incidence or severity of each of these sequelae; a recent clinical study demonstrated a modest benefit of cariporide (HOE 642) in patients with acute anterior myocardial infarction undergoing percutaneous transluminal coronary angioplasty (Rupprecht et al., 2000).
Zoniporide was recently identified as a novel, potent, and selective inhibitor of the human NHE-1 isoform (Guzman-Perez et al., 2001; R. B. Marala, J. A. Brown, J. X. Kong, W. R. Tracey, D. R. Knight, R. T. Wester, D. Sun, S. P. Kennedy, E. S. Hamanaka, R. B. Ruggeri, and R. J. Hill, submitted). In the present study, we evaluated the ability of this compound to provide cardioprotection from myocardial ischemic injury, both in vivo and in the isolated heart. Zoniporide produced a concentration- and dose-dependent reduction in myocardial injury, reducing infarct size by up to 83%, and demonstrated high potency (EC50 of 0.25 nM in the isolated heart). Furthermore, the cardioprotection observed in vivo occurred in the absence of any hemodynamic changes. In the in vivo preparation, inhibition of NHE-1 by zoniporide was confirmed by assessing exchanger function in platelets obtained from animals treated with the compound. Zoniporide dose dependently inhibited platelet NHE-1 function in vivo; the ID50 for inhibition of platelet swelling correlated well with the ED50 for in vivo cardioprotection (0.21 and 0.45 mg/kg/h, respectively).
Several modestly selective NHE-1 inhibitors have been described in the literature, including ethylisopropylamiloride, methylpropylamiloride, HOE 694, EMD 85131, and BIIB 513 (Counillon et al., 1993; Yasutake et al., 1994; Noel and Pouyssegur, 1995; Gumina et al., 1998, 1999). However, in recent years at least two NHE-1 inhibitors, cariporide (Graul et al., 1997; Rupprecht et al., 2000) and eniporide (Baumgarth et al., 1998), have entered clinical trials in patients with acute coronary syndrome. Zoniporide represents at least a 3-fold increase in NHE-1/NHE-2 selectivity over these compounds, and is also a more potent inhibitor of the NHE-1 isoform (Guzman-Perez et al., 2001; R. B. Marala, J. A. Brown, J. X. Kong, W. R. Tracey, D. R. Knight, R. T. Wester, D. Sun, S. P. Kennedy, E. S. Hamanaka, R. B. Ruggeri, and R. J. Hill, submitted). To compare the cardioprotective efficacy of zoniporide with cariporide and eniporide, these compounds were evaluated in the rabbit Langendorff model. We observed that zoniporide was more potent (EC50 and EC90) than either compound (2.5- and 20-fold versus eniporide and cariporide, respectively), and although equally efficacious to cariporide, both cariporide and zoniporide produced a greater reduction in infarct size relative to eniporide. In addition, the reduction in infarct size elicited by zoniporide compared favorably with the cardioprotection provided by ischemic preconditioning in these models (Tracey et al., 1997, 2000).
In summary, we have demonstrated that the novel NHE-1 inhibitor zoniporide produces a marked cardioprotection from ischemic injury both in vitro and in vivo, and represents a significant improvement in selectivity, potency, and in vitro cardioprotection over other known NHE-1 inhibitors. Zoniporide may prove clinically useful for reducing myocardial ischemic injury in acute coronary syndromes, in the high-risk surgical setting (peri-operative myocardial injury), and in secondary prevention in patients with ischemic heart disease. Potential clinical utility may also exist under conditions of ischemic injury to other organs or tissues, and during transplantation.
Acknowledgment
We acknowledge the expert technical assistance of Christian J. Mularski during the synthesis of zoniporide.
Footnotes
-
Send reprint requests to: W. Ross Tracey, Ph.D., Pfizer Global Research and Development, MS8220-3125 Eastern Point Rd., Groton, CT 06340. E-mail:w_ross_tracey{at}groton.pfizer.com
- Abbreviations:
- NHE
- sodium-hydrogen exchanger
- HR
- heart rate
- LVDP
- left ventricular developed pressure
- CF
- total coronary flow
- MAP
- mean arterial pressure
- RPP
- rate pressure product
- LV
- left ventricle
- % IA/AAR
- infarct area expressed as a percentage of area-at-risk
- % AAR/LV
- area-at-risk expressed as a percentage of left ventricular area
- PRP
- platelet-rich plasma
- Received October 23, 2000.
- Accepted January 8, 2001.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}