


Abstract
Intestinal disposition of small molecules involves interplay of drug metabolizing enzymes (DMEs), transporters, and host-microbiome interactions, which has spurred the development of in vitro intestinal models derived from primary tissue sources. Such models have been bioengineered from intestinal crypts, mucosal extracts, induced pluripotent stem cell (iPSC)–derived organoids, and human intestinal tissue. This minireview discusses the utility and limitations of these human-derived models in support of small molecule drug metabolism and disposition. Enteroids from human intestinal crypts, organoids derived from iPSCs using growth factors or small molecule compounds, and enterocytes extracted from mucosal scrapings show key absorptive cell morphology while are limited in quantitative applications due to the lack of accessibility to the apical compartment, the lack of monolayers, or low expression of key DMEs, transporters, and nuclear hormone receptors. Despite morphogenesis to epithelial cells, similar challenges have been reported by more advanced technologies that have explored the impact of flow and mechanical stretch on proliferation and differentiation of Caco-2 cells. Most recently, bioengineered human intestinal epithelial or ileal cells have overcome many of the challenges, as the DME and transporter expression pattern resembles that of native intestinal tissue. Engineering advances may improve such models to support longer-term applications and meet end-user needs. Biochemical characterization and transcriptomic, proteomic, and functional endpoints of emerging novel intestinal models, when referenced to native human tissue, can provide greater confidence and increased utility in drug discovery and development.
Introduction
Predicting pharmacokinetics and drug-drug interactions (DDIs: inhibition and induction) of novel small molecule therapeutics is an important consideration in drug discovery and development. Although the liver is known to be a predominant clearance organ, over time it has been increasingly accepted that the intestine also plays a major role in clearance (secretory), metabolism, and DDIs. As with the liver, numerous drug-metabolizing enzymes (DMEs) (phase I and II) and transporters, such as ATP binding cassette (ABCs) and solute-linked carriers (SLCs), reside in the gut and are loci of important DDIs as well as major determinants of intestinal extraction and oral bioavailability (Rogers et al., 1987). Thus, the gut is not simply an “absorption” organ; it is also regarded as an integral part of the enterohepatic axis and the site of host-microbiome interactions (Li et al., 2016; Malik et al., 2016).
Absorption (Fa) is a combination of solubility and permeability and can be predicted with confidence in humans (Artursson and Karlsson, 1991; Fagerholm, 2007; Wei et al., 2009) and rats (Nilsson et al., 2017). In contrast, discrete measurement of Fg, in vitro, has not been reported due to the lack of reliable assays derived from human intestinal sections. This is less of an issue for CYP3A substrates because of the availability of in vitro systems like human intestinal microsomes, S9 fractions, recombinant CYP3As, and in silico approaches (Gertz et al., 2011). One can scale the CYP3A turnover rate from these systems, using relative protein abundance or the relative activity factor to predict human intestinal intrinsic clearance (Paine et al., 1997). However, for non-CYP3A substrates, there are no suitable in vitro models that resemble the human intestinal apical environment experienced by novel, orally administered compounds. This is also convoluted by the heterogeneous expression of DMEs and transporters along the length of the human intestine (discussed later). Orally administered drugs undergo intestinal and hepatic metabolism in tandem, further complicating the separation of Fg from the fraction of the drug extracted from the liver into the systemic circulation. This has necessitated the development of in vitro models to support the study of drug metabolism and DDIs in the gastrointestinal tract, to derive in vitro–in vivo extrapolation (Jones et al., 2016), and to enable nonclinical screening of compounds.
Early attempts to study disposition of small molecules, in vitro, leveraged Ussing chambers (Wallon et al., 2005; Wuyts et al., 2015) with isolated human (endoscopic biopsied) tissue, followed by migration to gut tissue–derived subcellular fractions, and finally, the deployment of human gut “surrogate” reagents such as LS180 and Caco-2 cells (Rogers et al., 1987; Yamaura et al., 2016). Only recently has it been possible to consider using physiologically relevant human intestinal models by analogy with human primary hepatocytes [see Khetani et al. (2018) and Bale et al. (2018) in this special issue on novel models of drug metabolism, disposition, and toxicity]. Of late, several intestinal models bioengineered from induced pluripotent stem cells (iPSCs), crypts, mucosal extracts, and healthy human intestinal tissue have been reported. Although these models were initially developed to meet the needs of epithelial biologists to study gastrointestinal disorders like ulcerative colitis and Crohn’s disease, many of these models have recently been evaluated for expression and function of DMEs and transporters. This minireview discusses the state of the art and limitations of such emerging, primary, human-derived intestinal models to study disposition of small molecules. This minireview concludes with a framework describing end-user needs of drug metabolism scientists, validation endpoints, and computational parameters to enable scaling the outputs from preclinical discovery to development.
Anatomy of the Gastrointestinal Tract
The gastrointestinal tract consists of four layers of tissue (starting from the outside to inside), including the serosa, muscularis, submucosa, and mucosa (Mescher, 2018). The mucosa is the innermost layer enveloping the lumen and specializes in absorption and secretion. This innermost mucosal layer is lined by an epithelium, which displays distinct morphologies along each of the small and large intestinal sections. The small intestinal segments (duodenum, jejunum, and ileum), are arranged into invaginations (crypts) and finger-like protrusions (villi) that represent units specialized in the absorption of micronutrients (Elliott and Kaestner, 2015). The colon comprises the large intestine and consists of crypts; villi are absent in this region. Six differentiated cell types populate the crypt-villus axis of the intestinal epithelium. The most abundant cells are the enterocytes (i.e., absorptive cells) and goblet cells (i.e., mucus-secreting cells). Other, less abundant cell types include enteroendocrine cells that secrete gastrointestinal hormones, tuft cells thought to play a role in immune activation, M cells that deliver antigen to lymphoid tissues, and Paneth cells that localize at the base of the crypts and secrete antimicrobial peptides. With the exception of Paneth cells, which have a lifetime of approximately 2 months in the mouse (Ireland et al., 2005), all differentiated cell types in the human intestinal epithelium are short lived. Enterocytes, goblet cells, and the other secretory lineages are born in the crypts and migrate to the top of the villi over 5–7 days in humans and 3–5 days in mice, after which they are shed into the lumen of the intestine (Marshman et al., 2002; Barker et al., 2007; Clevers, 2013; Clevers and Batlle, 2013). Enterocytes expressed at the brush border or villi of the small intestinal wall are the major absorptive cells of the intestine, offering an enhanced surface area for absorption for drugs, xenobiotics, and nutrients. In addition to absorptive properties, these villi express DMEs and transporters responsible for carrier-mediated disposition at the epithelial barrier (Pang, 2003; Miyauchi et al., 2016).
Transcriptional and Proteomic Signatures of DMEs and Transporters in Human Intestinal Sections
mRNA expression and protein content of clinically relevant DMEs (https://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/) and transporters (Hillgren et al., 2013) as measured by immunoquantification, Western blotting, or liquid chromatography (LC)–tandem mass spectrometry (MS/MS) peptide quantification was published previously. Paine et al. (2006) reported the relative abundance of cytochrome P450 (P450) isozymes in duodenal and jejunal mucosal scrapings, using Western blotting; CYP3A and CYP2C9 were the most abundant P450 isozymes, accounting for 80% and 15% of total P450 content, respectively, followed by CYP2C19 > CYP2J2 > CYP2D6. By application of real-time polymerase chain reaction (RT-PCR) and LC-MS/MS (peptide quantification), Drozdzik et al. (2017) observed similar trends of P450 expression in biopsies from the human jejunum, ileum, and colon. In addition to CYP3A, CYP2C9/19, and CYP2D6, the authors also reported significant expression of UDP-glucuronosyltransferase (UGTs) 1A1/1A3 and 2B7 (Table 1). In addition, all detected enzymes confirmed the highest expression in the jejunum, with significant correlations between mRNA and protein levels for most enzymes.
Proteomic abundance of clinically relevant DMEs
Similar assessment of clinically relevant intestinal transporters (Hillgren et al., 2013), using quantitative LC-MS/MS assays and Western blotting, has been reported (Labroo et al., 1997; Paine et al., 2006; Tucker et al., 2012; Hillgren et al., 2013; Drozdzik et al., 2014, 2017; Nakamura et al., 2016; Akazawa et al., 2018). SLC15A1 [peptide transporter 1 (PEPT1)] has been consistently reported to be the most abundant jejunal transporter, whereas SLC10A2 (ASBT) showed the greatest variability across different gastrointestinal regions (Table 1). According to (Drozdzik et al., 2014; Drozdzik and Oswald, 2016), organic anionic transporting polypeptide 1A2 (OATP1A2) (mRNA and protein) is not detected in any intestinal segment. In contrast, multidrug resistance protein 3 (MRP3), organic cationic transporter 3 (OCT3), and, to a lesser extent, multidrug resistance protein 2 (MRP2) were more abundant in the colon than in the small intestine, whereas organic anion-transporting polypeptide 2B1 (OATP2B1) and organic cationic transporter 1 (OCT1) were uniformly expressed along the entire gut. All drug transporter protein abundances taken from individual reports are summarized in Table 2. Overall, region-specific expression of DMEs and drug transporters suggests that humanized systems designed to predict portal availability and intestinal, pharmacokinetic DDIs should be appropriately evaluated. Keeping in mind this heterologous expression pattern, this minireview will highlight opportunities for drug metabolism and transporter scientists offered by each of the systems discussed below.
Proteomic abundance of clinically relevant drug transporters
Enteroids
Some of the earliest human intestinal cultures were obtained from crypts isolated from intestinal tissue. Seminal work by Clevers (2013) demonstrated that under optimized media conditions, intestinal stem cells can form “mini-intestines” or enteroids, which differentiate into small intestinal villus-like or colonic cells consisting of enterocytes, goblet cells, enteroendocrine cells, and tuft cells (Mahe et al., 2015; Zachos et al., 2016). To date, there are no reports on expression of DMEs and transporters in human crypt-derived enteroids. However, Lu et al. (2017) recently explored expression of DMEs in enteroids derived from crypts isolated from wild-type and genetically modified murine intestine. This study demonstrated the expression of nuclear receptors [pregnane X receptor (Pxr), retinoid X receptor, constitutive androstane receptor, and peroxisome proliferator–activated receptor], P450 isozymes, carboxyl esterases (CESs), glutathione transferases (GSTs), and Ugts as well as drug transporters [P-glycoprotein (P-gp; Abcb1a), Mrp2 (Abcc2), and Abcg5/8]. The authors particularly explored functional activity of Ces and Ugt in these enteroids by determining Ces-catalyzed conversion of irinotecan to SN-38 (7-ethyl-10-hydroxycamptothecin) and Ugt-catalyzed detoxification of SN-38 to SN-38 glucuronide (Chen et al., 2013). Enteroids generated from Ugt1F/F mice efficiently generated SN-38 and SN-38 glucuronide; irinotecan-mediated cytotoxicity was observed at doses ranging from 10 to 100 μM. In contrast, enteroids from Ugt1ΔIEC mice showed that SN-38 mediated cytotoxicity at a 1 μM dose of irinotecan, due to depletion of Ugts. Similar trends in functional activity and cytotoxicity were also observed in enteroids generated from Ugt1F/F-deficient mice. This murine proof-of-concept report exemplifies a systematic approach to examine drug metabolism and toxicity of small molecules using enteroids. Although these enteroids may mimic human physiology by differentiating into key intestinal cell types, the apical compartment is not accessible, limiting the utility of this system to measure net extraction ratios across a typical intestinal epithelial bilayer. Lack of homogenous monolayers on a medium- to high-throughput device limits the scalability of these enteroids to discovery applications.
Enterocytes
Ho et al. (2017) and Yan et al. (2017) recently reported the isolation and cryopreservation of human intestinal enterocytes. In this model, enterocytes were produced by digesting the intestinal lumen, followed by differential centrifugation; enterocytes were cryopreserved for long-term storage. Functional activities of all major P450 isozymes, UGT, sulfotransferase (SULT), and CES2 were measured in this system by quantification of metabolites of specific probe substrates, using LC-MS/MS. Quantifiable activities were observed for CYP2C8, CYP2C9, CYP2C19, CYP2E1, CYP3A4, CYPJ2, CES2, UGT, and SULT, but not for CYP1A2, CYP2A6, CYP2B6, and CYP2D6; significant donor-to-donor variability was observed in the activities of P450 isozymes. Yan et al. (2017) subsequently characterized this system, as an in vitro model to assess intestinal clearance, by normalizing the functional activity of probe P450 substrates in enterocytes to that in hepatocytes. As expected, this normalization demonstrated that the functional activity of CYP3A4 was lower in enterocytes than in hepatocytes; however, the activity of UGTs (raloxifene hydroxylase) was 3-fold greater in enterocytes than in hepatocytes, which was unexpected. The authors also reported 9-fold lower activity of CES2 in enterocytes compared with that in hepatocytes and no turnover of salbutamol (a predominant SULT1A1 substrate). These cryopreserved enterocytes suppressed metabolism of loperamide (a CYP3A4/P-gp substrate) when treated with elacridar (CYP3A/P-gp inhibitor), suggesting that P-gp may not be functional in this system. Overall, this system is useful to determine the metabolism of predominant CYP3A substrates; absence of P-gp and breast cancer resistance protein (BCRP), as well as discrepancies in functional activities of DMEs expressed in this system, limits its utility to study non-CYP3A–mediated drug disposition. Additional optimization and transcriptional as well as proteomic characterization may enable quantitative scaling of CYP3A and other isozymes that are expressed in these cryopreserved enterocytes.
Induced Pluripotent Stem Cells (iPSCs)
Growth factor–directed differentiation of human pluripotent stem cells to functional enterocytes was first reported by Spence et al. (2011). Since then, several efforts have been undertaken to characterize iPSC-derived intestinal systems for biology and absorption, distribution, metabolism, and excretion (ADME) studies. Iwao et al. (2014) differentiated human iPSCs to functional enterocytes using epidermal growth factors, followed by maturation of the enterocytes using low serum concentration (2% fetal bovine serum). As determined using mRNA quantification, these mature enterocytes expressed SLC15A1/PEPT1 and CYP3A, with expression levels being 9- to 30-fold higher in differentiated versus nondifferentiated cells; however, the expression levels were reported to be lower than those observed in the adult intestine. Subsequently, Takenaka et al. (2014) reported an optimized monolayer of enterocytes differentiated from iPSCs to support longer-term cultures. Quantitative RT-PCR confirmed the mRNA of CYP3A5, UGT1A3, and UGT1A6; however, CYP3A4, CYP2D6, CYP2C19, and CYP2C9 were poorly expressed in this system. This system has expressed all major intestinal drug transporters, including OCT1, OATP2B1, monocarboxylate transporter 1, concentrative nucleotide transporter 3, equilibrative nucleoside transporters 1–3, P-gp, BCRP, and MRP1–MRP3, and the expression levels were similar to or approximately 10-fold higher than those in the human small intestine. Functional and inhibitable activity of P-gp (digoxin/verapamil) and BCRP (mitoxantrone/Ko143 [(3S,6S,12aS)-1,2,3,4,6,7,12,12a-octahydro-9-methoxy-6-(2-methylpropyl)-1,4-dioxopyrazino[1′,2′:1,6]pyrido[3,4-b]indole-3-propanoic acid 1,1-dimethylethyl ester]) was also confirmed in this system. Takenaka et al. (2014) showed that the monolayers in this system were “leaky” compared with Caco-2 monolayers, and the authors suggested that the transepithelial electrical resistance (TEER) in this system is closer to human intestinal TEER, with the caveat that TEER values in Caco-2 could be a function of cell source and experimental conditions; permeability measures of paracellular model compounds was higher than that observed in the parallel artificial membrane permeability assay and Caco-2 monolayer. Thus, although this system formed enterocyte monolayers that may enable high-throughput screening and expressed P-gp, BCRP, CYP3A5, UGT1A1, and UGT1A6, it may have limited applications in drug disposition due to lower expression levels of predominant DMEs, including CYP3A.
Iwao et al. (2015) reported pharmacokinetic enhancement in differentiated enterocytes by treatment with epidermal growth factors and small molecule enhancers Y-27632 [(1R,4r)-4-((R)-1-aminoethyl)-N-(pyridin-4-yl)cyclohexanecarboxamide], dorsomorphin, PD98059 [2-(2-amino-3-methoxyphenyl)4H-1-benzopyran-4-one], 5-aza-2′-deoxycitidine, and A-83-01 [3-(6-methyl-2-pyridinyl)-N-phenyl-4-(4-quinolinyl)-1H-pyrazole-1-carbothioamide]. Quantitative RT-PCR confirmed the mRNA levels of CYP3A, CYP2C, CYP2D, and PEPT1 genes. Similar efforts were reported by Kodama et al. (2016) using the following analogous small molecule regulators: mitogen-activated protein kinase, DNA methyltransferase, and transforming growth factor-β inhibitors. The authors reported that these regulators increased the expression of CYP3A and functional activities of CYP1A1/2, CYP2B6, CYP2C9, CYP2C19, CYP3A4/5, UGT, and SULTs. Interestingly, the CYP3A4 mRNA expression level was induced by treatment with 1α,25-dihydroxyvitamin D3 but not by treatment with rifampin, suggesting that the PXR pathway (and its downstream enzymes and transporters like P-gp) was not functional in this enterocyte model, which is a major limitation of this model. Subsequent efforts by Negoro et al. (2016) generated PXR-inducible CYP3A from mature human epithelial cell lines by overlaying Matrigel on the differentiated iPSC-derived enterocytes. The iPSC-derived mature enterocytes using Matrigel overlay successfully expressed nuclear receptors PXR, glucocorticoid receptor, and vitamin D receptor, as confirmed by treatment with rifampin, phenobarbital, 1α,25-dihydroxyvitamin D3, and dexamethasone. Treatment with dexamethasone, phenobarbital, rifampicin, or 1α,25-dihydroxyvitamin D3 resulted in approximately 5.8-fold, 13.4-fold, 9.8-fold, or 95.0-fold induction of CYP3A4 expression relative to that in the untreated controls, respectively. The levels of intestinal nuclear receptors PXR, glucocorticoid receptor, farnesoid X receptor, small heterodimer partner, and vitamin D receptor were also reported to be higher than in Caco-2 and LS180 cells. Similar improvement in expression of PXR-inducible CYP3A was reported by Ozawa et al. (2015), where enterocytes were derived from human iPSCs by using epithelial growth factors (epidermal growth factor, SB431542, and Wnt3A) and by extending the differentiation period. This treatment improved TEER and also resulted in increased gene expression of CYP3A4 and PEPT1. Most recently, Onozato et al. (2018) differentiated iPSCs using the small molecule compounds described previously (A-83-01, PD98059, and 5-aza-2′-deoxycytidine or 5-aza-2′-deoxycytidine plus DAPT, [N-[(3,5-difluorophenyl) acetyl]-L-alanyl-2-phenyl-1,1-dimethylethyl ester-glycine]), followed by seeding on EZSPHERE (San Diego, CA) plates to generate uniform spheroids. Treatment with these small molecule compounds expressed CYP3A4, PEPT1, OATP2B1, MRP2, BCRP, and P-gp; mRNA activities of CYP2C9, CYP2C19, and CYP2D6 were also detected in this system but expression of the apical sodium–dependent bile acid transporter (ASBT) (as measured via mRNA) was lower than that in the human adult intestine. Modest induction (mRNA and enzyme activity) of CYP3A4 was observed when treated with rifampicin and with 1,25-dihydroxyvitamin D3. Onozato and colleagues reported morphologic characterization of microvilli, as well as immunofluorescence staining of villin, and occludin; these results confirm the formation of tight junctions and a functional barrier, but permeability measurements across the bilayer have not been reported. Additional characterization of permeability and optimization of the inducible PXR pathway may enhance its utility for the study of intestinal disposition of drugs. In conclusion, small molecule compounds and growth factor–directed differentiation of human iPSCs can yield mature enterocytes expressing some of the DMEs or transporters; additional optimization could maximize the utility of such models in studying intestinal drug disposition.
Microfluidics-Based Platforms
Apart from small molecule cocktails, the impact of fluid flow and mechanical stretch on cell differentiation has recently been explored. Kim et al. (2012) investigated the effect of flow on proliferation and differentiation of Caco-2 cells. The authors reported that mechanical stretch differentiated Caco-2 cells into absorptive enterocytes and morphogenesis to form intestinal villi. In addition, CYP3A expression increased during villous formation but plateaued thereafter. Quantitation using the P450-Glo CYP3A4 assay demonstrated greater activity in this system compared with that in Caco-2 transwells. This activity was lower than that reported for human small intestinal microsomal fractions from human epithelial preparations (erythromycin N-demethylase activity: 0.30–0.76 nmol/min per milligram microsomal protein) by Zhang et al. (1999). This low CYP3A activity is probably due to the intrinsically low expression of CYP3A in Caco-2 cells. Functional activity and abundance of key intestinal transporters (P-gp, BCRP, PEPT1, ASBT) has not been reported in this system, limiting its use for drug disposition studies.
Similar efforts to build a microfluidic platform have been reported (Chen et al., 2017), in which human gut–liver tissue interactions were evaluated by an integrated multiorgan platform consisting of Caco-2–derived intestinal cultures differentiated into enterocytes, goblet cells, and dendritic cells. This system maintained barrier integrity over 2 weeks, as measured by TEER, and was comparable to previously reported TEER values for Caco-2 and HT29-MXT cocultures in transwell assays as well as primary intestinal monolayers (VanDussen et al., 2015). The same integrated gut–liver system was also applied by Tsamandouras et al. (2017a) to quantitatively measure the enterohepatic disposition of P450 substrates. Kinetics of diclofenac and hydrocortisone were investigated, followed by mechanistic modeling to determine the in vitro–to–in vivo correlation of this system. However, both of these systems have been derived from Caco-2 cell lines.
A significant development in studying ADME using primary cell-derived intestinal models was recently reported by Ayehunie et al. (2018). This is a microtissue system in which ileal epithelial cells and fibroblasts were expanded in a monolayer culture and seeded into single-well cell culture inserts or into a high-throughput 96-well membrane bottom plate for up to 42 days at the air liquid interface. The epithelial cells differentiated into Paneth cells, tuft cells, and Muc-2–positive goblet cells and enterocytes with villi-like brush border structures, as concluded by the authors. This system produces an average TEER value of 152.5 ± 39 Ω*cm2 in 96-well cultures and is able to functionally differentiate flux of high- versus low-permeability compounds. Immunohistochemistry and functional activity measured by concentration-dependent efflux of digoxin with or without verapamil confirmed P-gp expression on the apical surface. RNA levels of CYP3A4, CYP3A5, CYP2C9, and GSTs and key efflux transporters including P-gp/MDR1, MRP1, MRP-2, and BCRP were also confirmed using RT-PCR. P-gp/MDR1 was shown to be upregulated by >10-fold when cocultured with fibroblasts. The mRNA level of GSTs was comparable to that of native intestinal tissue.
This model is an important development because it simulates several structural, transporter, and metabolic features of the human ileum and can be used to measure permeability, P450-mediated metabolism, and P-gp/BCRP–mediated efflux of small molecules. A limitation of this system is the absence of SULTs and UGTs 1A1 and 2B7. Nevertheless, metabolism of CYP3A and CYP2C9 substrates can be predicted pending further validation of this model (discussed later). Further investigation of this system for functional activity of the clinically relevant P450s and transporters could enhance its application in drug disposition.
Most recently, Madden et al. (2018) reported the generation of human primary intestinal epithelial cells by “bioprinting” primary isolated epithelial cells. The intestinal tissue formed through this technique demonstrated a polarized epithelium with tight junctions. PXR, chicken xenobiotic receptor, CYP3A, CYP2C9, CYP2C19, CYP2D6, and CYP2J2 and phase II enzymes GSTP1 and UGT1A1 are expressed in this system. The initial expression data are promising; the activity of CYP3A across three donors tested in this study ranged from 2.85 to 19.3 pmol/min per milligram protein, which is lower than the previously published activity of CYP3A in human intestinal mucosal scrapings (8.8–150 pmol/min per milligram microsomal protein) (Paine et al., 2006). PXR-inducible CYP3A activity was confirmed by midazolam hydroxylation; this functional activity was comparable to that measured previously in intestinal tissue slices. Transcriptomic profiling also demonstrated the presence of P-gp, BCRP, PEPT1, OATP2B1, and ASBT. The authors concluded that the expression of these transporters was similar to that in native tissue preparations. Functional activity of P-gp and BCRP was determined by measuring the bidirectional transport of digoxin (Efflux ratio: 8.8) and topotecan (Efflux ratio: 190), which was inhibitable by zosuquidar. As such, absolute efflux ratios generated in an in vitro system generated at single concentrations can be best used to rank order compounds. Scaling functional activity from in vitro models to humans requires the magnitude of expression of the transporters as well as kinetics (Vmax and Km) of probe substrates. Overall, this system may become a suitable tool to study intestinal disposition of substrates of major DMEs and transporters, once characterized fully (as discussed later).
In summary, this minireview has discussed opportunities and limitations of enteroids, enterocytes, iPSC-derived enterocytes, bioengineered Caco-2 models, and human primary cell-derived models in studying in vitro intestinal drug disposition. Future models should be designed by leveraging the information gained from existing models and addressing gaps in the engineering and biochemical attributes experienced by the current models.
Engineering needs should consider a thermoplastic, optically clear, low nonspecific binding material; in addition, a bilayer design with access to the apical (top) and basolateral (bottom) chambers should be considered to enable direct, frequent, and easy sampling without perturbing the system; a bilayer design may also enable the introduction of specialized cell types like immune cells and macrophages, to measure disposition of novel therapeutics under diseased states. Similarly, extraction of monolayers and media from the top and bottom channels would allow for terminal readouts like RT-PCR and proteomics. It may also be desirable to have TEER sensors, oxygen control, and medium- to high-throughput capabilities. Biochemical characterization should consider discrete development of cell lines from different intestinal sections of primary human tissue (healthy or diseased). Technological advances like the introduction of flow and stretch may help duplicate the biology (Vedula et al., 2017; Bein et al., 2018). Longer-term applications of physiologically relevant intestinal systems derived from native tissue or iPSCs should be subject to quality controls to provide consistent differentiation and monolayer formation. Cell culture systems are developed by optimizing media conditions resulting in proprietary media which should be readily available, for scalability. Good viability (>75%) of cryopreserved enterocytes as well as human iPSC-derived enterocytes should be considered prior to experimentation (Ho et al., 2017). Continued optimization of primary human intestinal-derived cultures to yield a uniform monolayer with >90% viability of cryopreserved enterocytes is recommended.
Almost always, enterocyte cultures are or will be generated from multiple donors (8–10 per experiment) and from both sexes. As a result, donor-to-donor variability of ADME endpoints should be characterized prior to establishing cell lines for long-term usage. Intra- and interlot variability should be monitored after selection of lots that show good reproducibility; this initial quality control can ensure consistent delivery of routine, long-standing cultures. To measure DME and transporter activities, cells are typically incubated with probe substrates/inhibitors in culture media (approximately 150,000 cells/well of a 96-well plate) with incubation times ranging from 30 minutes to 3 hours (Ho et al., 2017; Yan et al., 2017); however, low-turnover compounds, need longer incubation times, to accurately measure the initial slope of elimination. Thus, method optimization should consider cell viability to be able to conduct experiments which may require prolonged incubation time. Reproducibility of a system can be ensured by studying at least three replicates and performing statistical analysis to define the variance and robustness of a system. Multiple quality controls, including RT-PCR, image-based readouts, and baseline levels of metabolic functions, should be implemented to assess good physiologic behavior of the systems.
Validation Criteria
Expression of intestinal DMEs and transporters requires differentiation of primary intestinal cells to enterocytes. Therefore, although it is not a necessity for an ADME scientist, differentiation of the human primary cells into absorptive enterocytes should be confirmed by immunohistochemistry of epithelial markers (namely, sucrose-isomaltase, alkaline phosphatase, or villin). Once the epithelial markers are established, tight junctions of the epithelial barrier should be confirmed using claudin staining, as this ultimately leads to increased confidence in the measurement of TEER (Mrsny et al., 2008; Landy et al., 2016). Finally, reproducible measurements of transcriptional, proteomic, and functional signatures of clinically relevant DMEs and transporters (Tables 1 and 2) in a humanized system enable the choice of the appropriate platform to meet end-user needs. Under the best-case scenario, transcriptional and proteomic signatures would be similar to those observed in human intestinal segments published by Drozdzik et al. (2014, 2017).
Design, Scaling Strategies, and In Vitro–In Vivo Extrapolation
Although scientists strive to derive a system that recapitulates physiologic abundance of DMEs and transporters, it should not be expected that these in vitro primary cell-derived systems will produce a quantitative output that is representative of intestinal permeability, metabolism, or transport and is translatable in vivo; additional scaling may be required. Central to this translation is the use of computational methodologies to integrate the operating characteristics of the in vitro system, such as the perfusion flow rate, number of cells in the incubation volume, nonspecific binding, population and relative ratio of different cell types, ratio of the tissue (cellular) volume to the volume of the surrounding medium, and residence time of chemical entities of interest within the system (Tsamandouras et al., 2017a,b). In addition to the integration of system parameters, robustly characterized proteomic, transcriptomic, and functional activities coupled with physiologically based pharmacokinetic approaches could enable appropriate scaling of the in vitro system.
In conclusion, we have reviewed the opportunities and limitations to study drug disposition, using recently published bioengineered models developed from Caco-2, iPSCs, mucosal scrapings, and human primary intestinal crypts. No single model meets all of the needs of drug metabolism scientists, due to limitations of each of the systems described in this minireview. Models described herein duplicate some of the enzymes and transporters expressed in human enterocytes and may need additional optimization for physiologic relevance as well as an improved throughout (medium to high). Engineering and biochemical attributes of future human-derived models should be designed, optimized, and scaled considering long-term, end-user needs and by evaluating endpoints discussed in Fig. 1.
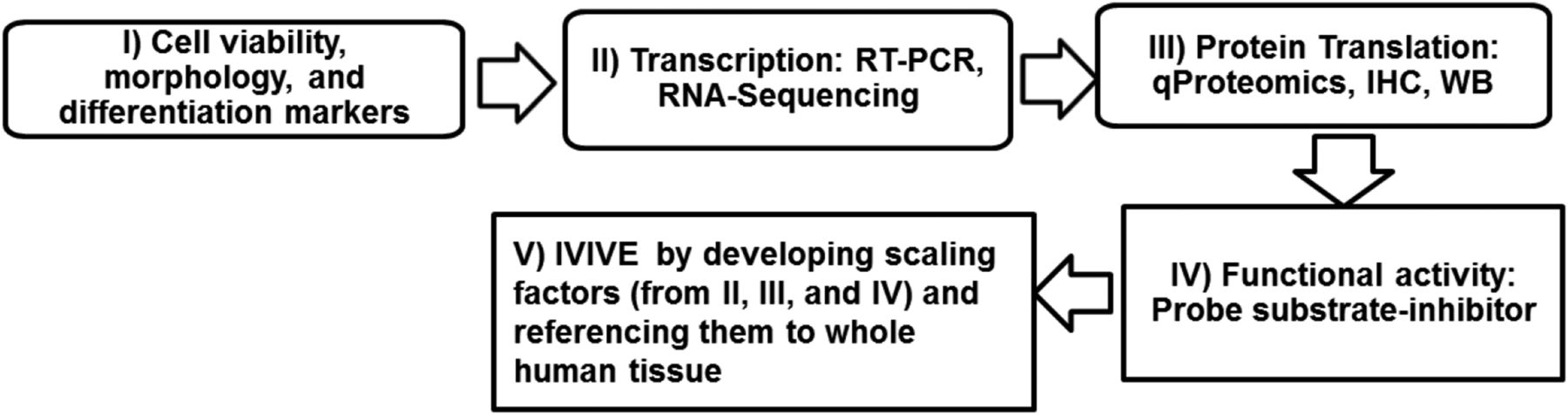
Proposed characterization and optimization of humanized intestinal in vitro models for drug disposition studies. IHC, immunohistochemistry; IVIVE, in vitro–in vivo extrapolation; WB, Western blotting.
Authorship Contributions
Wrote or contributed to the writing of the manuscript: Sawant-Basak, Rodrigues, Lech, Doyonnas, Kasaian, Prasad, Tsamandouras.
Footnotes
- Received June 1, 2018.
- Accepted August 16, 2018.
Abbreviations
- A-83-01
- 3-(6-methyl-2-pyridinyl)-N-phenyl-4-(4-quinolinyl)-1H-pyrazole-1-carbothioamide
- ABC
- ATP binding cassette
- ADME
- absorption, distribution, metabolism, and excretion
- ASBT
- apical sodium–dependent bile acid transporter
- BCRP
- breast cancer resistance protein
- CES
- carboxyl esterase
- DDI
- drug-drug interaction
- DME
- drug-metabolizing enzyme
- Fa
- fraction of the absorbed drug from the lumen into the enterocytes
- Fg
- fraction of the absorbed drug extracted from the gut into the portal vein circulation
- GST
- glutathione transferase
- iPSC
- induced pluripotent stem cell
- Ko143
- (3S,6S,12aS)-1,2,3,4,6,7,12,12a-octahydro-9-methoxy-6-(2-methylpropyl)-1,4-dioxopyrazino[1′,2′:1,6]pyrido[3,4-b]indole-3-propanoic acid 1,1-dimethylethyl ester
- LC
- liquid chromatography
- MRP
- multidrug resistance protein
- MS/MS
- tandem mass spectrometry
- OATP
- organic anionic transporting polypeptide
- OCT
- organic cationic transporter
- P450
- cytochrome P450
- PD98059
- 2-(2-amino-3-methoxyphenyl)4H-1-benzopyran-4-one
- PEPT
- peptide transporter
- P-gp
- P-glycoprotein
- PXR
- pregnane X receptor
- RT-PCR
- real-time polymerase chain reaction
- SLC
- solute-linked carrier
- SN-38
- 7-ethyl-10-hydroxycamptothecin
- SULT
- sulfotransferase
- TEER
- transepithelial electrical resistance
- UGT
- UDP-glucuronosyltransferase
- Y-27632
- (1R,4r)-4-((R)-1-aminoethyl)-N-(pyridin-4-yl)cyclohexanecarboxamide
- Copyright © 2018 by The American Society for Pharmacology and Experimental Therapeutics
References
In this issue





{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Anatomy of the Gastrointestinal Tract
- Transcriptional and Proteomic Signatures of DMEs and Transporters in Human Intestinal Sections
- Enteroids
- Enterocytes
- Induced Pluripotent Stem Cells (iPSCs)
- Microfluidics-Based Platforms
- Validation Criteria
- Design, Scaling Strategies, and In Vitro–In Vivo Extrapolation
- Authorship Contributions
- Footnotes
- Abbreviations
- References
- Figures & Data
- Info & Metrics
- eLetters