
Summary
The disposition of the lipid-lowering drug gemfibrozil was studied in patients with either renal (n= 8) or hepatic disease (n= 8) and compared to those of healthy volunteers (n= 6). Gemfibrozil was determined in plasma and urine by means of a HPLC method. Urine was also analyzed for gemfibrozil conjugates.
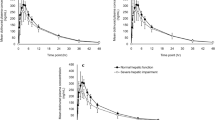
Following oral administration of 900 mg gemfibrozil, maximal plasma levels of the parent drug were 46.1±15.8 μg/ml, attained after 2.2±1.1 h. In chronic renal failure and in liver cirrhosis the plasma concentrations of gemfibrozil did not significantly differ from that of controls except in those patients who were comedicated with antacids. These patients had significantly lower Cmax and AUC values. The elimination half-life of the drug was 1.5 h in controls, 2.4 h in renal failure, and 2.1 h in liver disease. In healthy volunteers, only 0.02 to 0.15% of the given dose was recovered in the urine as parent gemfibrozil, while conjugates made up 7–14%. In patients with renal failure also, only traces of parent gemfibrozil could be detected, and conjugates accounted for 0.5–9.8%. In those with liver disease, however, about 0.1–0.2% were recovered in urine as parent gemfibrozil and up to 50% as conjugates. Strikingly, the amount of excreted conjugates in the urine was positively correlated to the direct bilirubin plasma concentration. It can be concluded that the elimination of gemfibrozil is not significantly influenced by renal failure. However, comedication with antacids markedly reduced plasma disposition of the drug. Patients with severe liver disease excreted more conjugated gemfibrozil via the kidney than did healthy controls. Thus, transfer across the canalicular cell membrane to the bile duct, rather than drug metabolization, is primarily disturbed in liver disease. Gemfibrozil accumulation is unlikely to occur in either kidney or liver disease.
Similar content being viewed by others
Abbreviations
- Clr :
-
creatinine clearance (ml/min)
- HPLC:
-
high pressure liquid chromatography
- Cmax :
-
maximal plasma concentration (μg/ml)
- tmax :
-
time (h) after which Cmax is attained
- ke :
-
elimination rate constant (h−1)
- t1/2 :
-
elimination half-life (h)
- Ae :
-
amount of drug excreted into the urine (% of given dose)
- MRT:
-
mean residence time (h)
- AUMC:
-
area under the first moment curve (μg h2/ml)
- AUC:
-
area under the plasma level time curve (μg·h/ml)
- ANOVA:
-
analysis of variance
References
Bennet WM (1981) Altering drug dose in patients with diseases of kidney and liver. In: Anderson RJ, Schrier RW (eds) Clinical use of drugs in patients with kidney and liver disease. Saunders, Philadelphia, pp 16–23
Buscher H-P, Fricker G, Gerok W, Kramer W, Kurz G, Müller M, Schneider S (1986) Membrane transport of amphillic compounds by hepatocytes. In: Greten H, Windler E, Beisiegel U (eds) Receptor-mediated uptake in the liver. Springer, Berlin Heidelberg, pp 189–199
Eisalo A, Manninen V, Mälkönen M, Kuhlbäck B (1976) Hypolipidemic action of gemfibrozil in adult nephrotics. Proc R Soc Med 69 [Suppl 2]:47–48
Frick MH et al. (1987) Helsinki Heart Study: primary prevention trial with gemfibrozil in middle-aged men with dyslipidemia. N Engl J Med 317:1237–1245
Gibaldi M, Perrier D (1982) Pharmacokinetics. Second Edition, Marcel Dekker, New York, p 409
Harvey SC (1980) Gastric antacids and digestants. In: Goodman LS, Gilman A (eds) The pharmacological basis of therapeutics, 6th edn. Macmillan, New York Toronto London, pp 988–1001
Hengy H, Kölle EU (1985) Assay of gemfibrozil in plasma by high performance liquid chromatography. Arzneimittelforschung/Drug Res 35 (II): 1637–1639
Jain AK, Ryan JR, Lacorte WSJ (1981) Clinical evaluation of gemfibrozil, a new antilipidemic agent. Clin Pharmacol Ther 29 (2): 254–255
Kaukola S, Manninen V, Mälkönen M, Enholm C (1981) Gemfibrozil in the treatment of dyslipidaemias in middleage male survivors of myocardial infarction. Acta Med Scand 209:69–73
Knauf H, Spahn H, Mutschier E (1989) Increased urinary excretion of diuretics in hepatitis patients. In: Puschet JB, Greenberg A (eds) Diuretics. Elsevier, New York Amsterdam London, pp 75–78
Manninen V, Mälkönen M (1982) Gemfibrozil treatment of dyslipidaemias in renal failure with uremia or in the nephrotic syndrome. Res Clin Forums 4:113–118
Manninen V, Mälkönen M, Eisalo A (1980) Is gemfibrozil safe for patients with renal disease? Abst. VII International Symp. Drugs Affecting Lipid Metab., Milan, p 26
Manninen V, Mälkönen M, Eisalo A, Virtamo J, Toumilehto J, Knusisto P (1982) Gemfibrozil in the treatment of dyslipidemia: a five-year follow-up study. Acta Med Scand (Suppl) 668:82–87
Mutschler E, Gilfrich HJ, Knauf H (1983) Pharmacokinetics of triamterene in healthy volunteers and patients with liver and kidney disease. Klin Wochenschr 61:883–891
Oberholm RA, Keeley FJ, Peterson FE, Glazko AJ (1976) The metabolism of gemfibrozil. Proc R Soc Med 69 [Suppl 2]: 11–14
Peabody HD Jr (1981) The treatment of primary hyperlipoproteinemia and coronary artery disease. The atherogenic connection. AV/MD Marketing Snc., 40 New York
Randinitis EJ, Kinkel AW, Nelson C, Parker TD (1984) Gas chromatographic determination of gemfibrozil and its metabolites in plasma and urine. J Chromatogr Biomed Appl 307:210–215
Rollins DE, Klaassen CD (1979) Biliary excretion of drugs in man. Clin Pharmacokin 4:368–379
Sachs L (1984) Statistische Auswertungsmethoden. Springer, Berlin Heidelberg New York Tokyo, S 410
Samuel P (1984) Efficacy of gemfibrozil as a lipid regulator in a patient population in the United States. Vascular Medicine. J Clin Angiol 2:8–15
Schwandt P, Weisweiler P, Neureuther G (1979) Serum lipidprotein lipids after gemfibrozil treatment. Artery 5:117–124
Silbernagel S (1985) Amino acids and oligopeptides. In: Seldin DW, Giebisch G (eds) The Kidney: physiology and pathophysiology. Raven Press, New York, pp 1677–1701
Smith TC (1976) Toleration and biovailability of gemfibrozil in healthy men. Proc R Soc Med 69 [Suppl 2]:24–27
Spahn H, Reuter K, Mutschier E, Gerok W, Knauf H (1987) Amiloride pharmacokinetics in renal and hepatic disease. Eur J Clin Pharmacol 33:493–498
Ullrich KJ, Rumrich G (1988) Contraluminal transport systems in the proximal renal tubule involved in secretion of organic anions. Am J Physiol 254:F453-F462
Van Dyke RW (1989) Mechanisms of digestion and absorption of food. In: Sleisenger MH, Fordtran JS (eds) Saunders, Philadelphia, pp 1062–1088
Weiner IM (1985) Organic acids and bases and uric acid. In: Seldin DW, Giebisch G (eds) The Kidney: physiology and pathophysiology. Raven Press, New York, pp 1703–1724
Author information
Authors and Affiliations
Additional information
The paper is gratefully dedicated to G.W. Löhr
Rights and permissions
About this article
Cite this article
Knauf, H., Kölle, E.U. & Mutschler, E. Gemfibrozil absorption and elimination in kidney and liver disease. Klin Wochenschr 68, 692–698 (1990). https://doi.org/10.1007/BF01667018
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01667018