Safety and efficacy of digoxin: systematic review and meta-analysis of observational and controlled trial data
BMJ 2015; 351 doi: https://doi.org/10.1136/bmj.h4451 (Published 30 August 2015) Cite this as: BMJ 2015;351:h4451
- Oliver J Ziff, academic foundation doctor12,
- Deirdre A Lane, lecturer in cardiovascular health13,
- Monica Samra, foundation doctor2,
- Michael Griffith, consultant electrophysiologist4,
- Paulus Kirchhof, professor of cardiovascular medicine13,
- Gregory Y H Lip, professor of cardiovascular medicine13,
- Richard P Steeds, consultant cardiologist4,
- Jonathan Townend, professor of cardiology14,
- Dipak Kotecha, clinician scientist in cardiovascular medicine1345
- 1University of Birmingham Centre for Cardiovascular Sciences, Birmingham, UK
- 2Royal Free London NHS Foundation Trust, London, UK
- 3Sandwell and West Birmingham NHS Trust, City Hospital, Birmingham, UK
- 4University Hospitals Birmingham NHS Trust, Birmingham, UK
- 5Monash Centre of Cardiovascular Research and Education in Therapeutics, Monash University, Melbourne, Australia
- Correspondence to: D Kotecha, University of Birmingham Centre for Cardiovascular Sciences, Medical School, Edgbaston, Birmingham B15 2TT d.kotecha{at}bham.ac.uk
- Accepted 13 August 2015
Abstract
Objective To clarify the impact of digoxin on death and clinical outcomes across all observational and randomised controlled trials, accounting for study designs and methods.
Data sources and study selection Comprehensive literature search of Medline, Embase, the Cochrane Library, reference lists, and ongoing studies according to a prospectively registered design (PROSPERO: CRD42014010783), including all studies published from 1960 to July 2014 that examined treatment with digoxin compared with control (placebo or no treatment).
Data extraction and synthesis Unadjusted and adjusted data pooled according to study design, analysis method, and risk of bias.
Main outcome measures Primary outcome (all cause mortality) and secondary outcomes (including admission to hospital) were meta-analysed with random effects modelling.
Results 52 studies were systematically reviewed, comprising 621 845 patients. Digoxin users were 2.4 years older than control (weighted difference 95% confidence interval 1.3 to 3.6), with lower ejection fraction (33% v 42%), more diabetes, and greater use of diuretics and anti-arrhythmic drugs. Meta-analysis included 75 study analyses, with a combined total of 4 006 210 patient years of follow-up. Compared with control, the pooled risk ratio for death with digoxin was 1.76 in unadjusted analyses (1.57 to 1.97), 1.61 in adjusted analyses (1.31 to 1.97), 1.18 in propensity matched studies (1.09 to 1.26), and 0.99 in randomised controlled trials (0.93 to 1.05). Meta-regression confirmed that baseline differences between treatment groups had a significant impact on mortality associated with digoxin, including markers of heart failure severity such as use of diuretics (P=0.004). Studies with better methods and lower risk of bias were more likely to report a neutral association of digoxin with mortality (P<0.001). Across all study types, digoxin led to a small but significant reduction in all cause hospital admission (risk ratio 0.92, 0.89 to 0.95; P<0.001; n=29 525).
Conclusions Digoxin is associated with a neutral effect on mortality in randomised trials and a lower rate of admissions to hospital across all study types. Regardless of statistical analysis, prescription biases limit the value of observational data.
Introduction
Heart failure and atrial fibrillation are two emerging epidemics of the 21st century. Despite considerable advances in the management of both conditions, there remain controversies regarding some of the most widely used drugs, including β blockers1 and cardiac glycosides.2 Digitalis, first introduced to clinical cardiology by William Withering in Birmingham around 1785, has widely been used as a positive inotrope in heart failure and for its negative chronotropic activity in atrial fibrillation. Recently, the use of digoxin has declined,3 4 5 partially because of concerns about safety after the publication of observational studies reporting increased mortality with digoxin.6 7 8 In contrast, the largest randomised controlled trial of digoxin in heart failure (the DIG trial) showed neutral effects on mortality and a reduction in admissions to hospital compared with placebo, as well as a decrease in mortality among those with low serum digoxin concentrations.9 10 The results of several smaller randomised trials were consistent with these findings, showing that digoxin improves symptoms and prevents clinical deterioration.11
In atrial fibrillation, however, no such experimental trials exist, and confusion about whether digoxin is truly linked to adverse prognosis has led to the downgrading of digoxin in clinical practice guidelines.12 13 14 Two recent meta-analyses have supported this view but were based solely on a small selection of observational studies,15 16 highlighting the need for a more comprehensive assessment. Furthermore, the finding that β blockers have no prognostic impact in patients with heart failure and concomitant atrial fibrillation1 has again led to questions as to what alternatives clinicians have available. There is therefore a clear imperative to define the place of digoxin in the clinical management of both heart failure and atrial fibrillation and to guide physicians and patients with an indication for treatment with digoxin.
Digoxin is particularly prone to prescription bias as clinicians have been trained to use digoxin in sicker patients. Statistical adjustment of observational data does not remove all confounding, and even techniques such as propensity score matching cannot replace randomised allocation.17 18 19 Different types of adjustment for confounders often result in conflicting findings, adding to confusion for clinicians. For example, with the same dataset, three post hoc analyses of the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) trial reported different conclusions regarding the safety of non-randomised prescriptions of digoxin.20 21 22
In view of the potential usefulness of digoxin in heart failure and atrial fibrillation, and in an attempt to settle the uncertainty over adverse outcomes, we assessed the efficacy and safety of digoxin by comprehensively meta-analysing all available observational and experimental studies. Our hypothesis was that study design would have an important impact on the observed mortality associated with digoxin.
Methods
Eligibility criteria and search strategy
We evaluated all studies that examined comparative outcomes with digoxin and control (placebo or no treatment), regardless of study design. All cardiovascular outcomes and all populations were included. We excluded studies that did not provide comparative outcomes or were not published as full text articles in English. The definitions of heart failure, atrial fibrillation, coronary artery disease, and myocardial infarction used by each individual study were accepted. We systematically reviewed Medline (1960 to July 2014), Embase (1980 to July 2014), and the Cochrane Library (until July 2014 Issue). The search strategy included keywords and MeSH terms relating to cardiac glycosides and death, admission to hospital, or other cardiovascular outcomes. We also manually searched reference lists of relevant studies, investigated registers of ongoing trials, and included studies after discussion with content experts.
The review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.23 The project was prospectively registered with the PROSPERO database of systematic reviews (CRD42014010783).24
Data collection, synthesis, and risk of bias
Two investigators (OJZ and MS) independently extracted and tabulated data on a standardised data extraction form. Discrepancies and missing data were resolved by group discussion, reference to the original publication, and additional independent adjudication (DK). All data were extracted from studies, including crude outcome data and adjusted analyses, comprising multivariate adjustment and propensity matched data, where available. Careful note was made of the analysis method (including risk ratio (preferred), odds ratio, or hazard ratio) and the population studied. Additional unpublished data were provided from the authors of two studies on clinical outcomes of interest .25 26 Studies by Freeman and colleagues27 and Whitbeck and colleagues20 were excluded from the quantitative meta-analysis as digoxin was assessed in a time dependent fashion, whereas all other studies assessed digoxin at baseline. Jorge and colleagues28 and Domanski and colleagues29 were not meta-analysed as crude event rates were not presented. Gheorghiade and colleagues21 and Whitbeck and colleagues20 provided unadjusted data derived from the same cohort (the AFFIRM trial), albeit with different patient inclusion. We performed a sensitivity analysis and inclusion/exclusion of one or the other study had no effect on results. Ancillary analyses of trials were not included if the original study reported mortality outcomes for the whole population. When more than two treatment arms were assessed, we incorporated only the digoxin and placebo treatment effects.30 31 We also included two studies in press at the July 2014 cut-off date; both were subsequently published in full.7 8
We assessed the risk of bias with the Cochrane Collaboration’s risk of bias tool for randomised controlled trials and the risk of bias assessment tool for non-randomised studies (RoBANS), both of which address key criteria such as selection bias, exposure measurement, blinding, completeness of outcome data, and selectivity of reporting.32 33 We assessed of risk of bias using these standardised tools independently from data extraction, with each study assessed by two authors and adjudication by a third when required.
Primary and secondary outcomes
The predefined primary outcome was all cause mortality. Secondary outcomes included cardiovascular mortality; admission to hospital for any cause, cardiovascular causes, and heart failure; incident stroke; and incident myocardial infarction. We also explored evidence for a dose related effect on outcomes.
Statistical analysis
We meta-analysed baseline demographics, comparing the digoxin and control groups from all studies that provided unadjusted data, and summarised them as the weighted mean difference or odds ratio. Meta-analysis was prespecified to use a random effects model because of the anticipated variety in study designs and populations. Pooled binary event data for digoxin and control cohorts were compared with risk ratios and associated 95% confidence intervals with the method of DerSimonian and Laird.34 In cases where the odds ratio was described, we converted these to a risk ratio for meta-analysis (RR=OR/([1−pRef]+[pRef*OR]), where pRef is the prevalence of the outcome in the reference group).35 Results provided as hazard ratios were meta-analysed separately from risk ratios.
Outcomes were assessed according to type of analysis (unadjusted, adjusted, propensity matched, and randomised controlled trials) and the population studied (heart failure and/or atrial fibrillation, or other populations including unspecified). Because of the small number of trials available for analysis of admission to hospital, we performed two exploratory meta-analyses that included various study types. We assessed these with a fixed effects approach according to the method of Mantel and Haenszel,36 with confirmation using the random effects model previously described. Sensitivity analyses were performed according to study design and by subpopulations, including a post hoc defined assessment in patients with concomitant heart failure and atrial fibrillation.
Heterogeneity was assessed with χ2 squared test and I2 statistic, with the estimate of heterogeneity taken from the inverse variance fixed effects model. Meta-regression was performed to assess the impact of baseline variables on the logarithm of effect estimates of crude unadjusted mortality outcomes from observational data. The primary assessment used the residual maximum likelihood with random effects weighting and the Knapp and Hartung t-distribution.37 To avoid false positive results, we confirmed our findings using the method of moments, with P value calculation from 20 000 random Monte Carlo permutations.38 An exploratory meta-regression was performed according to the risk of bias attributed to each study. Publication bias was assessed with Begg’s test and Egger’s test to identify small study effects according to study analysis methods and also in the overall cohort disregarding study design. A two tailed P=0.05 was considered significant. Analyses were performed with Stata Version 13.1 (StataCorp LP, TX).
Results
The search strategy identified 52 studies for systematic review, including 621 845 patients allocated to digoxin treatment or control, representing 2 248 775 patient years of follow-up (fig 1).⇓ Overall, 144 593 patients were taking digoxin (23.3%) compared with 476 984 in the control arms (76.7%). Study descriptors are summarised in table A in appendix 1. Of the 42 studies, 26 were retrospective or prospective cohorts,6 7 25 28 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 nine were post hoc analyses of randomised trials,20 21 60 61 62 63 64 65 66 and seven were randomised on the basis of digoxin.9 30 31 67 68 69 70 The length of follow-up (weighted average) was 3.7 (SD 2.4) years with a range of 0.25-8.2 years.

Fig 1 Selection of studies flowchart (after duplicates removed) on safety and efficacy of digoxin. *Primary outcome (all cause mortality) includes data from 41 studies
{kind=link}
Table 1⇓ summarises the differences in key characteristics between digoxin and control groups (for full baseline demographics, see table B in appendix 1). Patients receiving digoxin were older than controls (weighted mean difference 2.4 years), more likely to be diabetic, and more often receiving diuretics or anti-arrhythmic drugs. Sample size weighting suggested that mean left ventricular ejection fraction was lower in digoxin patients (0.33) than controls (0.42). We were unable to meta-analyse left ventricular ejection fraction because of a lack of data on standard deviation.
Pooled weighted characteristics of baseline demographics in patients treated with digoxin compared with control. Figures are odds ratio (95% CI) unless stated otherwise
The risk of bias in individual studies is presented in tables C and D in appendix 1. As expected, this was proportional to the robustness of study design, with randomised controlled trials having the lowest risk of bias. There was no evidence of small study effects or publication bias in any of the analysis groups individually or when we combined all studies using the most adjusted analysis available (all P>0.1 for Begg’s and Egger’s tests).
Meta-analysis was suitable for five outcomes: all cause mortality, cardiovascular mortality, all cause hospital admissions, cardiovascular hospital admissions, and heart failure hospital admissions.
All cause mortality
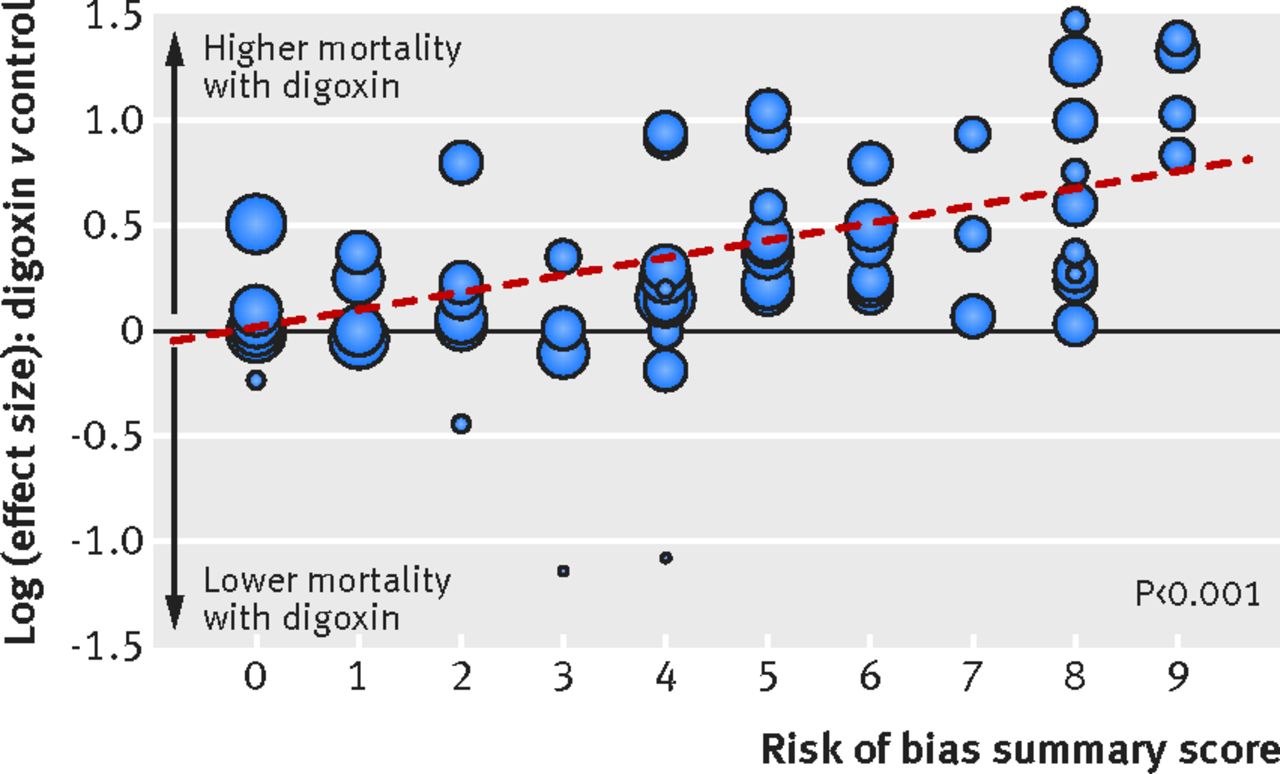
Forty one studies were suitable for meta-analysis of all cause mortality.6 7 8 9 20 21 25 26 30 31 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 These studies contributed to 75 separate analyses, with an overall combined total of 999 994 patients and 4 006 210 patient years of follow-up across four analysis subtypes (table 2⇓). Figure 2 presents a summary of the individual meta-analyses performed⇓. We performed an exploratory meta-regression of the effect of study level bias on all cause mortality for digoxin compared with control. This analysis confirmed that studies with higher bias reported a greater association of digoxin with death (P<0.001; fig 3⇓ and table 3).⇓ Appendix 2 shows results of studies not included in the meta-analysis.

Fig 2 Summary of meta-analyses for all cause mortality in observational and randomised studies on safety and efficacy of digoxin, comprising 999 994 participants across 75 study analyses. (See fig 4 and figs A, C, D, and E in appendix 3 for study level results)
{kind=link}

Fig 3 Meta-regression of all cause mortality according to risk of bias and efficacy of digoxin. Risk of bias in each study was summed across all six domains (low risk=0, unclear risk=1, high risk=2; excluding “other threats to validity” domain from Cochrane risk of bias tool). All analyses that provided data on rates of death were included, regardless of study design. Each circle represents particular study, with circle size dependent on precision of each estimate in random-effects model (inverse of its variance)
{kind=link}
Summary of studies and patients in systematic review and meta-analyses of safety and efficacy of digoxin
Meta-regression for all cause mortality in studies on safety and efficacy of digoxin
Unadjusted data from observational studies
Unadjusted mortality rates for digoxin and control were available in 33 observational analyses (n=331 935).6 7 8 20 21 25 26 39 40 41 42 43 44 45 46 47 49 50 51 52 53 55 56 57 58 59 60 61 62 63 64 65 66 The risk ratio for all cause mortality was 1.76 (95% confidence interval 1.57 to 1.97; P<0.001; fig A in appendix 3). There was substantial heterogeneity across trials (>90%; P=0.001). In studies pertaining only to heart failure and/or atrial fibrillation cohorts, the risk ratio was 1.33 (1.19 to 1.50; P<0.001) compared with 2.61 (2.12 to 3.22; P<0.001) for other patient populations. In 28 studies that provided crude event numbers, 18 161/69 763 (26.0%) patients died in the digoxin group compared with 37 563/200 266 (18.8%) in the control arm.
Meta-regression was used to explore the impact of differences in key baseline characteristics between digoxin and control patients on all cause mortality in observational data. Studies with smaller differences in the percentage of patients with diabetes, as well as those receiving diuretics and anti-arrhythmic drugs, reported less difference in mortality between digoxin and control. At study level, baseline age and year of publication also significantly affected the comparative risk of death between patients treated with digoxin and control (table 3⇑ and fig B in appendix 3).
Adjusted data from observational studies
Adjusted mortality data were available for 22 observational analyses (n=245 049).7 21 26 41 42 43 44 45 47 50 53 55 56 57 58 59 62 63 65 66 Compared with control, digoxin was associated with an increased risk of death (risk ratio 1.61, 95% confidence interval 1.31 to 1.97, P<0.001; hazard ratio 1.17, 1.07 to 1.29, P=0.001; see fig C in appendix 3). In studies that enrolled only patients with heart failure and/or atrial fibrillation, the risk of death associated with digoxin use was of borderline significance (hazard ratio 1.16, 1.05 to 1.28; P=0.04). Adjustment factors varied widely (table E in appendix 1).
Propensity matched observational studies
Thirteen analyses (n=414 604) used a propensity matched cohort design.6 7 8 21 46 48 56 57 58 67 Compared with control, digoxin use was associated with a small increased risk of death in studies that reported risk ratio (1.18, 95% confidence interval 1.09 to 1.26; P<0.001). There was no significant association in studies that reported hazard ratios (1.07, 0.96 to 1.19; P=0.20; fig D in appendix 3). In studies of patients with heart failure and/or atrial fibrillation, there were similar results for risk ratios (1.18, 1.10 to 1.27; P<0.001), but no difference in mortality for studies reporting hazard ratios (1.00, 0.84 to 1.20; P=0.99).
Randomised controlled trials
Seven randomised controlled trials were included (n=8406).9 30 31 67 68 69 70 There were no differences in mortality between patients randomised to digoxin or placebo (risk ratio 0.99, 95% confidence interval 0.93 to 1.05; P=0.75; fig 4⇓). All seven of these trials were conducted in patients with heart failure. Importantly, there was no evidence of heterogeneity across studies (I2=0%, P=0.97).

Fig 4 Meta-analyses of all cause mortality in randomised controlled trials on safety and efficacy of digoxin
{kind=link}
All cause mortality in patients with heart failure and atrial fibrillation
We performed a post hoc defined sensitivity analysis to assess the impact of digoxin on mortality in patients with combined heart failure and atrial fibrillation, which included two analyses of crude observational data,46 55 two adjusted observational analyses,55 59 and two propensity matched cohorts8 46 (total n=46 274; 139 769 patient years of follow-up). Digoxin had no significant effect on mortality in this patient group (see fig E in appendix 3). These studies included patients with a clinical heart failure syndrome, although on the basis of average left ventricular ejection fraction, most patients had heart failure with reduced ejection fraction.
Cardiovascular mortality
Limited data were available for cardiovascular mortality. In patients with heart failure and/or atrial fibrillation, five randomised studies (n=8068) found no association between use of digoxin and cardiovascular death (risk ratio 1.01, 95% confidence interval 0.94 to 1.08; P=0.82).9 31 67 69 70 In contrast, pooled data from one adjusted and two unadjusted observational studies in other patient populations (n=11 399) found an increased risk of cardiovascular death (2.53, 1.12 to 5.71; P=0.025).39 45 63
Admission to hospital, other cardiovascular events, and digoxin dose
Detailed results on admissions to hospital and other outcomes are presented in appendix 2. To summarise, digoxin was associated with a small but significant reduction in all cause admission to hospital across all study types (overall risk ratio 0.92, 95% confidence interval 0.89 to 0.95; P<0.001; fig F in appendix 3), as well as significantly lower rates of admissions related to cardiovascular disease and heart failure (see fig G in appendix 3). There was no evidence for any increase or reduction in other cardiovascular events with digoxin, such as myocardial infarction or incident stroke. Limited information on digoxin dose suggests that lower serum digoxin concentrations of between 0.5 and 0.9 ng/mL were associated with improved prognosis, whereas higher concentrations correlated with increased mortality.
Discussion
Digoxin has a neutral effect on all cause mortality in randomised trials and is associated with a reduction in hospital admission. This finding is based on a comprehensive systematic review including over 600 000 patients, with meta-analysis incorporating a combined total of four million patient years of follow-up. Based on our analysis, observational studies that report increased mortality with digoxin use (regardless of statistical methods) were unable to adjust for systematic differences in the type of patients who received digoxin. Uniquely, we were able to show that studies exhibiting a higher risk of bias reported a stronger association with all cause mortality, highlighting the need to base clinical decisions relating to patient management on high quality data derived from controlled trials, rather than post hoc or observational data.
Heart failure and atrial fibrillation cause a substantial burden of disease worldwide.71 72 Throughout most of the past century, digoxin was routinely used to improve cardiac output and to avoid admission to hospital. Based on information from large randomised trials, the use of digoxin has been eclipsed by the widespread initiation of drugs with prognostic benefit, including ACE inhibitors73, β blockers (in sinus rhythm),1 and aldosterone antagonists.74 75 This decline in use followed evidence from the DIG Trial that digoxin does not reduce mortality in patients with heart failure,9 despite high rates of concomitant digoxin use in most trials of treatment for heart failure. Currently, European and American guidelines recommend digoxin for persistent symptoms, despite optimal treatment, or as an alternative/adjunct to reduce hospital admissions.76 77 Atrial fibrillation guidelines preferentially suggest treatment with β blockers over digoxin, except in sedentary patients or as an adjunct for additional rate control.13 78
Heart failure and atrial fibrillation often co-exist, leading to further adverse prognosis.79 80 81 A recent individual patient data meta-analysis showed that β blockers had no significant effect on mortality or hospital admission in patients with heart failure and reduced ejection fraction and concomitant atrial fibrillation.1 In this context, clinicians have only a single other choice of rate control treatment—namely, digoxin—as calcium channel blockers can have negatively inotropic effects in failing hearts.82 83 In this increasingly prevalent population, our findings regarding digoxin might be of particular clinical importance. Our analysis confirmed that, similar to β blockers, digoxin has a neutral effect on mortality in patients with co-existing heart failure and atrial fibrillation, even in observational studies with associated prescription biases. Although there were insufficient data to assess hospital admissions specifically in patients with heart failure plus atrial fibrillation, we found that digoxin reduced admissions for any cause, cardiovascular causes, and heart failure across all study types. Whether digoxin has other beneficial effects, such as an increase in left ventricular ejection fraction or improvement in quality of life, has yet to be determined in patients with atrial fibrillation (for example, the proposed RAte control Therapy Evaluation in Atrial Fibrillation [RATE-AF] randomised trial84). This type of information is vital if we are to defend against the enormous healthcare burden posed by these two conditions.85 86
As digoxin is no longer first line treatment for either atrial fibrillation or heart failure, it is often prescribed when clinicians detect deterioration in patients resistant to initial treatment. Thus, treatment with digoxin is likely to be influenced by the probability of mortality, creating a scenario of “confounding by indication.”87 We have clearly shown the profound differences in baseline characteristics between patients in digoxin and control groups in observational studies and exposed their impact on all cause mortality through meta-regression methods. These differences could partly explain the conflicting results from recent observational studies derived from similar cohorts,20 21 22 a problem not unique to cardiology trials.88 89 The disparity in these studies promotes the notion that even sophisticated statistical methods should be interpreted with caution and cannot replace randomisation. Although statistical adjustment for known confounders is often used to combat allocation bias (for example, with propensity matching), important confounders can be unknown or masked. Even with a reasonable selection of adjustment variables, when treatment and control groups differ vastly in characteristics, reliable effect estimates are not possible without breaching the assumptions of the statistical model.90 91 92 With regards to digoxin, our analysis shows that adjustment for known confounders mitigates bias to an extent but will leave residual confounding that results in important clinical impact. Although digoxin has a higher tendency to such bias than other treatments, the same principle will apply to other cardiovascular treatments, providing a cautionary reminder that observational data are hypothesis generating, rather than definitive.
Several additional studies in patients with atrial fibrillation were published during the analysis stage of our study, and these are highlighted in table F in appendix 1. All were either post hoc assessments of trials or cohort/registry studies.93 94 95 96 97 98 99 One study found a lower death rate in patients treated with digoxin, three identified no association, and four identified higher mortality in patients treated with digoxin. In all studies there were substantial differences in the patients receiving digoxin compared with those receiving control treatment, including higher rates of heart failure, more advanced atrial fibrillation, prognostically worse baseline demographics, and receipt of drugs that have previously been associated with increased mortality, including anti-arrhythmic drugs. Taking all studies into account, our systematic review suggests that digoxin should continue to be considered as a treatment option to achieve control of heart rate in those with atrial fibrillation and also to avoid hospital admissions in patients with heart failure (fig 5)⇓. Despite our reassuring data with respect to mortality, clinicians should adhere to guidelines—for example, by ensuring the use of recommended drugs and devices in patients with heart failure and reduced ejection fraction, and appropriate anticoagulation in those with atrial fibrillation.

Fig 5 Overview of evidence base for digoxin versus placebo/no treatment
{kind=link}
Limitations
Our review is based on reported results of independent published studies, prepared according to explicit reproducible methods. Although meta-analysis of individual patient data is the ideal,100 it is practically unfeasible with such large combinations of data across an extensive number of studies. We acknowledge several limitations of our analysis. Firstly, there is a clear and understandable discrepancy in the sample sizes from randomised and observational data. Secondly, both heart failure and atrial fibrillation have a wide clinical spectrum, from asymptomatic disease to a severe uncontrolled condition. Definitions of heart failure and atrial fibrillation in different studies varied, and we cannot exclude misclassification. Although some studies reported the stage of heart failure, left ventricular ejection fraction, and the type of atrial fibrillation, many studies did not.
Thirdly, because of anticipated differences in study design and populations, we prespecified a random effects model. Although we noted substantial heterogeneity for all cause mortality between observational trials, this was not evident in meta-analysis of randomised controlled trails. We were unable to perform meta-analysis of serum digoxin concentration, digoxin dose, or the type of cardiac glycoside prescription (digoxin, digitalis, or digitoxin) because of insufficient data in the included studies. Of note, a large placebo controlled randomised trial has recently started recruitment, examining the effect of digitoxin in patients with heart failure and reduced ejection fraction.101 Although we found no evidence of publication bias, statistical measurements can be misleading especially when heterogeneity is high.102
Finally, because of a lack of randomised data in patients with atrial fibrillation without heart failure, we are unable to comment on the prognostic impact of digoxin specifically in these patients. Observational data here are limited as between 30% and 50% of patients with atrial fibrillation also have heart failure,79 and heart failure with preserved ejection fraction in particular is underdiagnosed.103 Although we saw no increase in mortality in patients with a clinical diagnosis of heart failure and concomitant atrial fibrillation, further randomised data are awaited in patients with atrial fibrillation to settle this important clinical question.
Conclusion
Digoxin use has a neutral effect on mortality in randomised trials and reduces hospital admissions. The association between digoxin and adverse outcomes in observational studies is likely to be non-causative and a result of confounding that cannot be mitigated by statistical adjustment. Future randomised trials of digoxin are urgently required to identify the place of this treatment in the management of patients with heart failure and those with atrial fibrillation.
What is already known on this topic
Digoxin is often used to reduce symptoms in patients with heart failure, as well as to control heart rate in those with atrial fibrillation
Recent observational studies have suggested increased mortality associated with digoxin, but these are limited by prescription bias, as only those patients at highest risk tend to receive digoxin
What this study adds
Our study comprehensively assessed data on mortality and cardiovascular outcomes from all studies since 1960 comparing the use of digoxin versus placebo or no treatment
Using meta-analysis and meta-regression techniques, we have highlighted the importance of basing treatment decisions on randomised controlled trial data, rather than observational studies, which are unable to correct for inherent bias
Notes
Cite this as: BMJ 2105;351:h4451
Footnotes
Contributors: DK designed the study concept, led the study group, performed statistical analysis, drafted the manuscript, and is guarantor. OJZ developed eligibility criteria, performed the primary literature search, contributed to data extraction, and drafted the manuscript. DAL, MS, MG, PK, GYHL, RPS, and JT contributed to data extraction and critical revision of the manuscript.
Funding: The study was funded by a grant from the Arthur Thompson Trust, University of Birmingham.
Competing interests: All authors have completed the ICMJE uniform disclosure form (www.icmje.org/coi_disclosure.pdf) and declare: DAL has received investigator initiated grants from Boehringer Ingelheim, Bayer Healthcare, and Bristol-Myers Squibb; personal fees from Bristol-Myers Squibb, Boehringer Ingelheim, and Bayer; non-financial support from Boehringer Ingelheim; and is a steering committee member of a phase IV study sponsored by Bristol-Myers Squibb. PK has received grants and personal fees from several research funders including European Union, British Heart Foundation, German Research Foundation, Leducq Foundation, German Ministry of Education and Research, NIHR, and from medical device and pharmaceutical companies. PK also has patents pending for atrial fibrillation therapy and markers. GYHL has served as a consultant for Bayer, Astellas, Merck, AstraZeneca, Sanofi, Bristol-Myers Squibb-Pfizer, Biotronik, Portola, and Boehringer Ingelheim, and has been on the speakers’ bureau for Bayer, Bristol-Myers Squibb-Pfizer, Boehringer Ingelheim, and Sanofi-Aventis. JT has received research funding and travel grants from AstraZeneca. DK is the lead for the Beta-blockers in Heart Failure Collaborative Group (BB-meta-HF), has received honorariums from Menarini and professional development support from Daiichi-Sankyo.
Ethical approval: Not required.
Transparency: The lead author (the manuscript’s guarantor) affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned and registered have been explained.
Data sharing: No additional data are available, though details on statistical analysis are available from the corresponding author on request.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.