


Abstract
Troglitazone sulfate (TGZS) is the major metabolite of troglitazone (TGZ), an antidiabetic agent, and thought to be a cause of the cholestasis induced by TGZ. The aim of the present study is to elucidate the involvement of breast cancer resistance protein (BCRP/ABCG2) in the hepatic disposition of TGZS. The basal-to-apical transport of TGZS was enhanced in organic anion transporting polypeptide 1B1-expressing Madin-Darby canine kidney II cells by infection of recombinant adenovirus harboring human BCRP and mouse Bcrp cDNA. TGZS was given to wild-type and Bcrp (–/–) mice by constant infusion. Biliary excretion is the predominant elimination pathway of TGZS in wild-type mice, and the biliary excretion clearance of TGZS with regard to the hepatic concentration was reduced to 30% of the control in Bcrp (–/–) mice. However, plasma and hepatic concentrations were unchanged, suggesting induction of compensatory mechanisms in Bcrp (–/–) mice for the elimination of TGZS. Involvement of BCRP in the intestinal efflux transport of TGZS was examined using everted sacs. The mucosal efflux clearance of TGZS showed only a slight reduction (15% reduction) in Bcrp (–/–) mice. Our results suggest that BCRP plays a major role in the biliary excretion but a minor role in the intestinal transport of TGZS.
Troglitazone (TGZ) (Fig. 1a) was the first marketed thiazolidinedione, and it has been used for the treatment of type 2 hyperglycemia. It can sensitize tissues to insulin by activating peroxisome proliferator-activated receptor-γ, thereby inhibiting glucose release from hepatocytes and enhancing the insulin-dependent glucose metabolism in adipose tissue and skeletal muscle (reviewed in Chen, 1998). However, TGZ was withdrawn from the market in 2000 because of idiosyncratic severe hepatotoxicity. A great deal of research was carried out on the hepatotoxicity of TGZ, and multiple mechanisms were proposed, such as the production of reactive intermediates and direct mitochondrial injury (reviewed in Smith, 2003). An alternative mechanism that has been proposed is cholestasis. Cholestasis was observed in patients with severe hepatotoxicity (Fukano et al., 2000; Menon et al., 2001), and Funk et al. (2001b) showed that a single bolus administration of TGZ increased the plasma bile acid concentration in rats. Because troglitazone sulfate (TGZS) (Fig. 1b), the major metabolite of TGZ, is a more potent inhibitor of the bile salt export pump (BSEP) than TGZ, and the hepatic concentration of TGZS was much greater than that of TGZ (Funk et al., 2001b), TGZS has been hypothesized to account for the cholestatic effect of TGZ. A gender difference in the cholestatic effect of TGZ in rats was related to the sex-dependent formation of TGZS: the formation of TGZS was greater in male rats, which exhibit more severe cholestasis (Funk et al., 2001a). Based on these findings, it has been speculated that TGZS increases the likelihood of hepatotoxicity induced by TGZ. In addition to the conjugation rate, the hepatic elimination mechanism of TGZS will be important for hepatotoxicity. Elucidation of the molecular mechanism of the hepatic disposition of TGZS is also important to obtain a clue to account for the idiosyncratic hepatotoxicity of TGZ. Polymorphisms or mutations of the enzymes and transporters may be associated with this idiosyncrasy.
TGZS is produced mainly by sulfotransferase (SULT) 1A1 in the liver and is predominantly excreted into the bile (Kawai et al., 1997; Honma et al., 2002). Almost 50% was recovered in the bile as unchanged form after intraduodenum administration of TGZS in rats (Kawai et al., 2000). As far as hepatic uptake is concerned, Nozawa et al. (2004) showed that TGZS is transported by organic anion transporting polypeptide (OATP) 1B1 and OATP1B3, and OATP1B1 transported TGZS more efficiently than OATP1B3 (Nozawa et al., 2004). OATP1B1 will play a major role in the hepatic uptake of TGZS. As far as the biliary excretion process is concerned, Kostrubsky et al. (2001) investigated the involvement of multidrug resistance-associated protein 2 (MRP2/ABCC2) in the biliary excretion of TGZS using TR– rats, a mutant strain with an inherited deficiency in MRP2. The biliary excretion of TGZS was delayed in TR– rats compared with normal rats; however, the amount of TGZS excreted into the bile was not markedly reduced in TR– rats (Kostrubsky et al., 2001). One explanation of this is that other transporters are also involved in the biliary excretion of TGZS. The transport system involved in the intestinal reabsorption of TGZS remains to be identified.

Chemical structures of TGZ (A) and TGZS (B).
Breast cancer resistance protein (BCRP/ABCG2) is a member of the ATP-binding cassette transporter family. BCRP is ubiquitously expressed in normal tissues, and cumulative studies using Bcrp (–/–) mice have shown the importance of BCRP in the urinary excretion, secretion into milk and tissue, and fetal distribution of xenobiotics (Maliepaard et al., 2001; Jonker et al., 2002, 2005). In the liver and intestine, BCRP is localized in the canalicular and brush-border membranes, respectively, and it mediates the biliary excretion of nitrofurantoin and pitavastatin and limits the oral absorption of topotecan, 2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine, and ME3277 (Jonker et al., 2002; van Herwaarden et al., 2003; Hirano et al., 2005; Kondo et al., 2005; Merino et al., 2005). The substrate specificity of BCRP is characterized by the acceptance of a variety of sulfate conjugates (Suzuki et al., 2003), and BCRP plays a significant role in the efflux transport of certain kinds of sulfate conjugates in the small intestine and kidney (Mizuno et al., 2004; Adachi et al., 2005). Therefore, we hypothesized that BCRP plays a critical role in the prevention of TGZ-induced cholestasis by facilitating biliary excretion, and investigated the contribution of BCRP to the biliary and intestinal excretion of TGZS using Bcrp (–/–) mice.
Materials and Methods
Materials and Animals. TGZ and TGZS were gifts from Sankyo Co. Ltd. (Tokyo, Japan). All the other chemicals were commercially available and of reagent grade. A 24-well Transwell (6.5-mm diameter, 0.4-μm pore size) was purchased from Corning Costar (Bodenheim, Germany). Male Bcrp (–/–) mice (Jonker et al., 2002) and wild-type FVB mice used in the present study were 9 to 16 weeks old and weighed 25 to 33 g. The animals were maintained under controlled temperature with a light/dark cycle of 12 h. Food and water were available ad libitum.
Transcellular Transport Study. The transcellular transport study was performed as previously reported with minor modifications (Matsushima et al., 2005). In brief, Madin-Darby canine kidney II (MDCKII) cells expressing human OATP1B1 (MDCKII/OATP1B1) were grown on the Transwell membrane for 3 days in Dulbecco's modified Eagle's medium (Invitrogen, Carlsbad, CA) with 10% fetal bovine serum (Sigma-Aldrich, St. Louis, MO) and 1% antibiotic-antimycotic solution (Sigma-Aldrich). The cells were infected with the recombinant adenovirus harboring green fluorescent protein (GFP), mouse Bcrp (mBcrp), or human BCRP (hBCRP) expression vector at an infection multiplicity of 200. The details of the construction of these recombinant adenoviruses were described in a previous report (Kondo et al., 2004). After 2 days of culture, the cells were used for transport studies. The cells were preincubated in Krebs-Henseleit buffer (142 mM NaCl, 23.8 mM Na2CO3, 4.83 mM KCl, 0.96 mM KH2PO4, 1.20 mM MgSO4, 12.5 mM HEPES, 5 mM glucose, and 1.53 mM CaCl2, pH 7.4) for 30 min, and then transport experiments were initiated by replacing the medium on one side of the cell monolayer with Krebs-Henseleit buffer containing 3 μM TGZS. At appropriate times (1, 2, and 3 h), 100-μl aliquots were taken from the opposite side of the cell monolayer and replaced with 100 μl of buffer. After the last sampling, the cell monolayers were solubilized with 500 μl of 0.2 M NaOH and then neutralized with 100 μl of 1 M HCl. The protein concentration was measured by the Lowry method.
The flux of TGZS across cell monolayers was calculated as follows: Flux (μl/mg protein) = (Cacceptor× Vacceptor)/(Cdonor× protein amount), where Cacceptor is the TGZS concentration in the acceptor solution, Vacceptor is the volume of the acceptor solution, and Cdonor is the initial TGZS concentration in the donor solution (3 μM). The flux was plotted against time, and the efflux clearances (μl/h/mg protein) were calculated from the slopes.
Determination of Biliary Excretion of TGZS in Wild-Type and Bcrp (–/–) Mice. Under urethane anesthesia (1.25 g/kg, i.p.), the right jugular vein was cannulated with a polyethylene tube (PE-10; Becton Dickinson, Franklin Lakes, NJ) for injection of TGZS. After abdominal dissection, the gallbladder was ligated, and the bile duct was cannulated with a polyethylene tube (UT-3; Unique Medical, Tokyo, Japan) to collect bile. TGZS was injected at a dose of 0.5 μmol/kg, followed by continuous infusion at a dose rate of 0.1 μmol/h/kg. Blood samples were collected from the left jugular vein at 60, 80, 100, and 120 min. The blood samples were heparinized and centrifuged to obtain plasma samples. Bile samples were collected at 20-min intervals between 60 and 120 min postdosing. Immediately after the last blood and bile sampling, mice were sacrificed, and the liver was removed. The liver was homogenized with a 9-fold volume of phosphate-buffered saline (PBS) to obtain a 10% liver homogenate.
The plasma samples (5 μl) were mixed with 20 μl of PBS and 75 μl of acetonitrile; the bile samples (1 μl) were mixed with 49 μl of PBS and 100 μl of acetonitrile; and the liver homogenates (10 μl) were mixed with 40 μl of PBS and 100 μl of acetonitrile. All these mixed solutions were centrifuged at 15,000g for 10 min. The supernatants (plasma sample, 80 μl; bile and liver sample, 10 μl) were evaporated, and the pellets were reconstituted with 20% acetonitrile (plasma sample, 80 μl; bile and liver sample, 200 μl) and subjected to liquid chromatography/mass spectrometry (LC/MS) analysis.
Determination of Urinary Excretion of TGZS in Wild-Type and Bcrp (–/–) Mice. Under urethane anesthesia (1.25 g/kg, i.p.), the right jugular vein was cannulated with a polyethylene tube (PE-10) for injection of TGZS, and the urinary bladder was cannulated with two polyethylene tubes (PE-50; Becton Dickinson). One cannula was fitted with a syringe filled with saline to wash the inside of the urinary bladder, and the other cannula was used for the collection of urine and wash solution. TGZS was injected at a dose of 0.5 μmol/kg followed by continuous infusion at a dose rate of 0.1 μmol/h/kg. Mannitol was concomitantly infused at a dose rate of 160 mg/h/kg to increase the urine volume. Urine samples were collected at 20-min intervals between 60 and 120 min. After every collection of urine, the bladder was flushed with about 300 μl of saline, and the wash solution was added to the urine. The urine samples (50 μl) were mixed with 150 μl of acetonitrile and centrifuged at 15,000g for 10 min. The supernatants (100 μl) were evaporated, and the pellets were reconstituted in 20% acetonitrile (100 μl) and subjected to LC/MS analysis.
Everted Sac Study. Mice were anesthetized with ether and sacrificed by exsanguination from the femoral artery and vein. Immediately after sacrifice, the ileum was dissected. The ileum was ligated at one end and then everted. The open end of the everted ileum was ligated after the insertion of a polyethylene tube (SP-45; Natsume, Tokyo, Japan) to make a 5-cm-long sac. Krebs-Ringer buffer (350 μl) containing 0.3% bovine serum albumin (BSA-KRB, pH 6.4) was added to the serosal side of the everted sac via the cannula, and the everted sacs were incubated at 37°C in 10 ml of BSA-KRB. After a 10-min preincubation, the everted sacs were placed in BSA-KRB containing 10 μM TGZ and incubated again at 37°C. Aliquots (200 μl) were collected from the mucosal side at 15, 30, 45, and 60 min after incubation with TGZ. After the last sampling, the serosal solution was removed, and the everted sacs were rinsed with ice-cold PBS. Throughout the entire procedure, the mucosal solution was bubbled with O2/CO2 (95:5) gas.

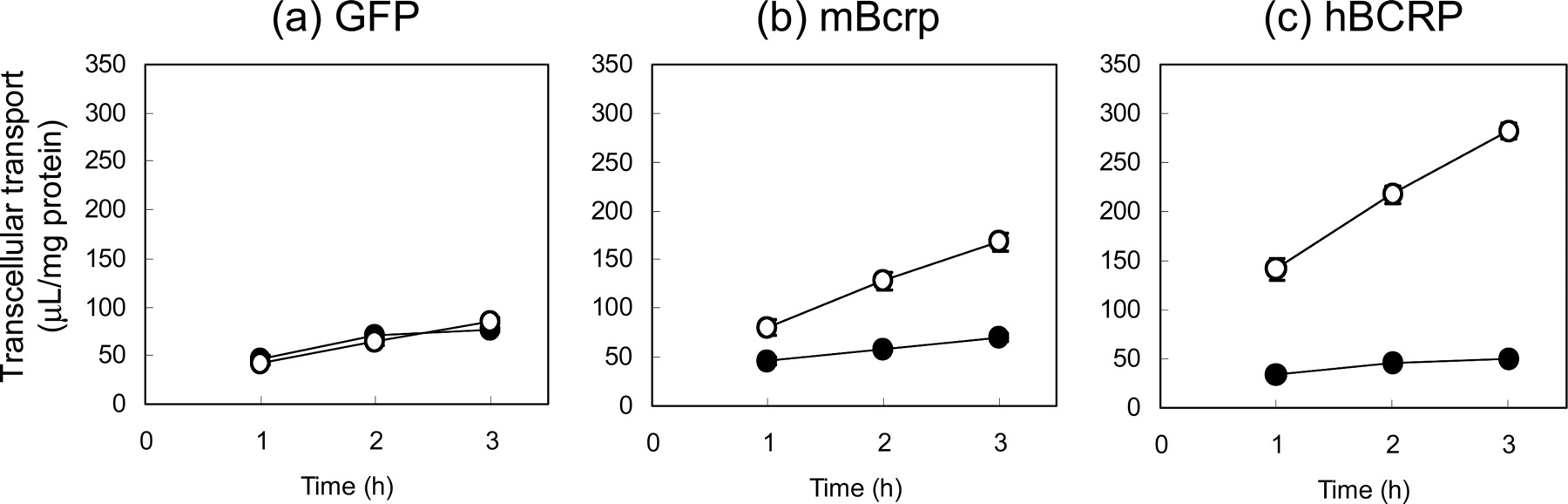
The transcellular transport of TGZS across monolayers of MDCKII/OATP1B1 expressing GFP, mBcrp, and hBCRP. The transport in the apical-to-basal direction is represented by closed circles and that in the basal-to-apical direction by open circles. Data are represented by mean values ± S.E. of triplicate experiments.
The aliquots (75 μl) from the mucosal solution were mixed with acetonitrile (75 μl) and centrifuged at 15,000g for 10 min. The supernatants were subjected to LC/MS analysis. The tissue samples were weighed and homogenized with a 9-fold volume of PBS to give 10% tissue homogenates. The tissue homogenates (50 μl) were mixed with acetonitrile (75 μl) and centrifuged at 15,000g for 10 min, and the supernatants were subjected to LC/MS analysis.
LC/MS Analysis. An LC/MS-2010 EV equipped with a Prominence LC system (Shimadzu, Kyoto, Japan) was used for the analysis. Samples were separated on a CAPCELL PAK C18 MGII column (3 μm, 2 × 50 mm; Shiseido, Tokyo, Japan) in binary gradient mode. For the mobile phase, 10 mM acetic ammonium and acetonitrile were used. The acetonitrile concentration was initially 23%, then linearly increased up to 70% over 1.5 min, and kept at 70% for a further 1 min. Finally, the column was re-equilibrated at an acetonitrile concentration of 23% for 2.5 min. The total run time was 5 min. TGZS was eluted at 3 min using this method. In the mass analysis, TGZS was detected at a mass-to-charge ratio of 520 under negative electron spray ionization conditions. The interface voltage was –3.5 kV, and the nebulizer gas (N2) flow was 1.5 l/min. The heat block and curved desolvation line temperatures were 200 and 150°C, respectively.
Data Analysis of Biliary Excretion. Because the plasma and biliary excretion was almost constant between 60 and 120 min (Fig. 3), the plasma and liver concentrations at 120 min were assumed to be steady-state concentrations. Total clearance (CLtot) was calculated by dividing the infusion rate by the plasma concentration at 120 min. The biliary excretion clearance based on the plasma concentration (CLbile, plasma) was calculated by dividing the biliary excretion rate in the last time segment (100–120 min) by the plasma concentration at 120 min. The biliary excretion clearance based on the liver concentration (CLbile, liver) was calculated by dividing the biliary excretion rate in the last time segment by the liver concentration at 120 min. The fraction of the biliary excretion was calculated by dividing the biliary excretion rate in the last time segment by the infusion rate.
Efflux Transport in Everted Sac Study. The mucosally excreted amounts of TGZS per unit length of tissue were calculated as follows: Mucosal excretion = (Cmucosal× Vmucosal)/tissue length, where Cmucosal is the TGZS concentration in the mucosal solution, Vmucosal is the volume of the mucosal solution (10 ml), and the tissue length was 5 cm. The excreted amounts of TGZS in the mucosal side were plotted against the incubation time (Fig. 4a), and the mucosal efflux rates were estimated from the slope. Mucosal efflux clearances (CLmucosal) were calculated by dividing the mucosal efflux rates by the tissue concentrations assuming that 1 g of intestine = 1 ml.
Statistical Analysis. Statistical analysis for significant differences was performed using the two-tailed Student's t test or one-way analysis of variance, followed by the Tukey multiple comparison test. A probability of <0.05 was considered to be statistically significant.
Results
In Vitro Transport Study of TGZS in BCRP-Expressed Cells. BCRP-mediated transport of TGZS was examined using GFP-, mBcrp-, and hBCRP-expressed MDCKII/OATP1B1 cells. Figure 2 shows the time courses of the transcellular transport of TGZS in GFP-, mBcrp-, and hBCRP-expressed cell systems. The transport of TGZS increased linearly up to 3 h, suggesting that the initial rates were maintained up to the end of the experiments. The transport rates are summarized in Table 1. The apical-to-basal transport was significantly reduced in hBCRP-expressed cells compared with that in GFP cells. The basal-to-apical transport was significantly increased in both mBcrp- and hBCRP-expressed cells. The ratios of basal-to-apical/apical-to-basal flux were 3.6 and 9.3 in MDCK II cells expressing OATP1B1/mBcrp and OATP1B1/hBCRP, respectively, whereas that in GFP-expressed cells was almost symmetric (flux ratio was 1.45).
Kinetic parameters of the transcellular transport of TGZS across the monolayers of MDCKII/OATP1B1 cells expressing GFP, mBcrp, and hBCRP
The data are represented by mean values ± S.E. of triplicate experiments. Statistical significance was analyzed by one-way analysis of variance followed by Tukey multiple comparison test.
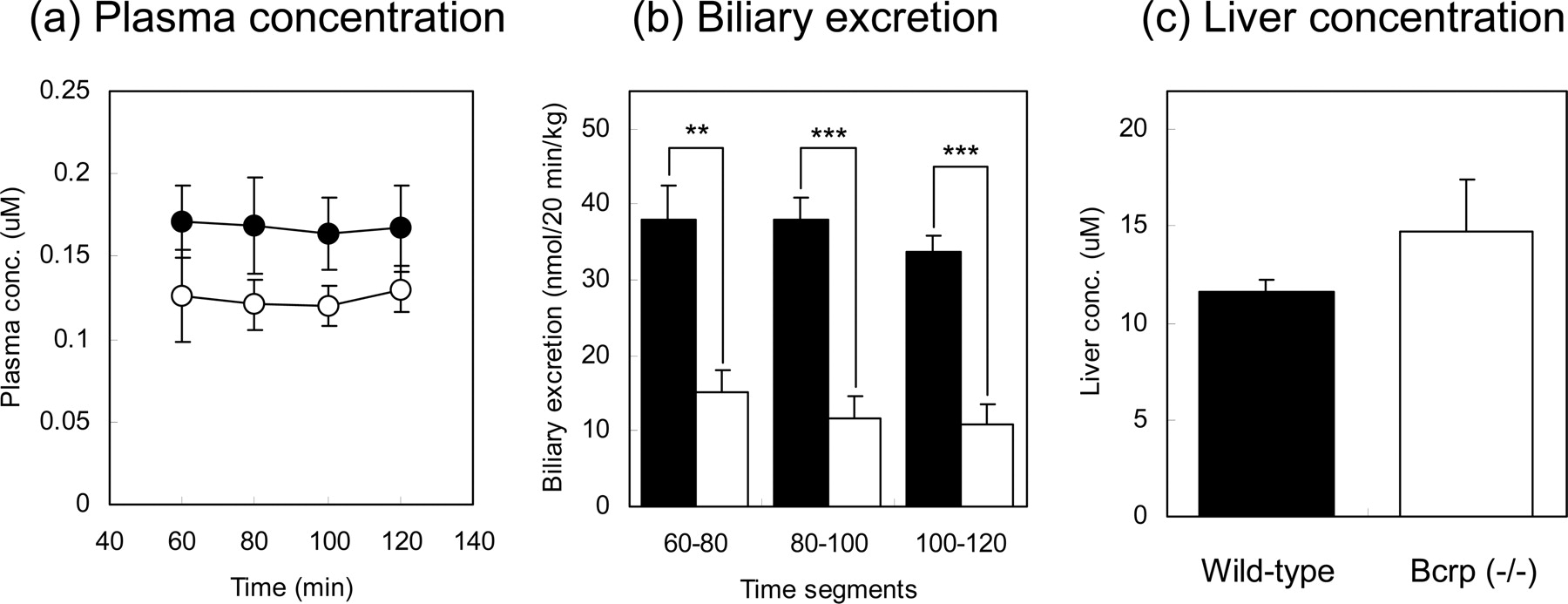
Effect of BCRP on the Biliary Excretion of TGZS. The biliary excretion study was performed by continuous infusion with a priming dose to achieve steady-state conditions. The biliary excretion, plasma, and liver concentrations of TGZS are shown in Fig. 3. The bile flow was almost the same in wild-type and Bcrp (–/–) mice (38.5 ± 4.6 versus 41.8 ± 5.4 μl/min/kg). The plasma concentrations and the biliary excretion of TGZS became almost constant between 60 and 120 min. The plasma concentrations showed a slight reduction in Bcrp (–/–) mice; however, the differences were not statically significant. The biliary excretion of TGZS was markedly reduced in Bcrp (–/–) mice at all the time periods. There was no significant difference in the liver concentrations between wild-type and Bcrp (–/–) mice. The pharmacokinetic parameters are shown in Table 2. The total clearance was slightly increased in Bcrp (–/–) mice, but this was not statistically significant. The biliary excretion clearances based on the plasma and liver concentrations were markedly reduced in Bcrp (–/–) mice to about 30% of those in wild-type mice. The biliary excretion of TGZS was almost 100% in wild-type mice, whereas that in Bcrp (–/–) mice was 32.6%. These results indicate that there is another elimination process for TGZS in Bcrp (–/–) mice. To investigate this, the urinary excretion of TGZS was examined in Bcrp (–/–) mice. However, TGZS concentrations in all the urine samples were below the lower limit of quantification (10 nM). Because the volume of the urine sample (urine + wash solution) was less than 450 μlat every 20-min period, the urinary excretion rate of TGZS was considered to be less than 0.45 nmol/h/kg. This means that the urinary excretion of TGZS is less than 1% of the dose in Bcrp (–/–) mice.
Pharmacokinetic parameters of TGZS in the in vivo biliary excretion study
The data are represented by mean values ± S.E. of four mice.

The effect of BCRP on the biliary excretion of TGZS. a, the time courses of the plasma concentrations of TGZS. b, the biliary excretion of TGZS. c, the liver concentrations of TGZS at 120 min postdosing. The data in wild-type mice are shown by closed circles or columns and those in Bcrp (–/–) mice by open circles or columns. All the data are represented by mean values ± S.E. of four mice. Asterisks represent statistically significant differences between wild-type and Bcrp (–/–) mice; **, P < 0.01 and ***, P < 0.001.
Effect of BCRP on the Mucosal Efflux Transport of TGZS in Everted Sacs. The effect of BCRP on the mucosal efflux transport of TGZS was examined by using everted ileum sacs. TGZ was added to the mucosal side, and the mucosal efflux of the intracellularly formed TGZS was determined. The results are shown in Fig. 4. The time courses of the mucosal efflux of TGZS were linear, suggesting that the initial rates were maintained up to the end of the experiments. The mucosal efflux was slightly reduced in Bcrp (–/–) mice (Fig. 4a). The tissue concentrations of TGZS at the end of the experiments were similar between wild-type and Bcrp (–/–) mice (Fig. 4b). The mucosal efflux clearance showed a significant but only slight reduction (15.3% decrease) in Bcrp (–/–) mice (Fig. 4c).
Discussion
The present study is focused on the involvement of BCRP in the biliary and intestinal excretion of TGZS. We first examined whether TGZS is a substrate of BCRP in vitro using a BCRP-expressed MDCKII/OATP1B1 system where OATP1B1 and BCRP are localized in the basal and apical membrane, respectively, and the basal-to-apical transport of their common substrates is increased (Matsushima et al., 2005). Compared with GFP-expressed cells, the basal-to-apical transport was increased in mBcrp- and hBCRP-expressed cells, suggesting that TGZS is a substrate of both mBcrp and hBCRP. A higher flux ratio was observed in hBCRP-expressed cells than in mBcrp-expressed cells, suggesting that hBCRP transports TGZS more efficiently than mBcrp.
In the in vivo study, there was no significant difference in bile flow between in wild-type and Bcrp (–/–) mice. The bile flow obtained in the present study was about 40 μl/min/kg and within the range of previously reported bile flows in FVB male mice (28.7 and 61 μl/min/kg) (Wang et al., 2001; Werner et al., 2002). These results suggested that cholestasis was not induced under the present experimental conditions. Funk et al. (2001b) showed the cholestatic effect of TGZ in rats. In that report, the plasma and liver concentrations of TGZS were 110 and 260 μM, respectively, much higher than those in the present study (plasma, 0.1–0.2 μM; liver, 10–15 μM). This suggests that the plasma and liver concentrations of TGZS in the present study were too low to induce cholestasis.
Comparison of the total body and biliary excretion clearances showed that biliary excretion is the main elimination pathway of TGZS in wild-type mice. The biliary excretion of TGZS was markedly reduced in Bcrp (–/–) mice, and CLbile, liver, which represents the intrinsic efflux ability at the canalicular membrane, was reduced in Bcrp (–/–) mice to 29% of that in wild-type mice. Therefore, BCRP is the major transporter involved in the biliary excretion of TGZS. Cumulative studies using Mrp2-deficient mutant rats have shown that MRP2 accounts for the biliary excretion of some sulfate conjugates, such as tauro-conjugated bile acid sulfate, phenolphthalein sulfate, and acetaminophen sulfate (Takikawa et al., 1991; Akimoto et al., 2001; Tanaka et al., 2003; Zamek-Gliszczynski et al., 2005). Very recently, Zamek-Gliszczynski et al. (2006) showed that BCRP is also involved in the biliary excretion of sulfate conjugates, including 4-methylumbelliferone sulfate, acetaminophen sulfate, and harmol sulfate, using Bcrp (–/–) mice. These results suggest that BCRP and MRP2 are two major transporters responsible for the biliary excretion of sulfate conjugates, and BCRP makes a major contribution to the biliary excretion of xenobiotic sulfate conjugates. In humans, the biliary excretion of TGZS may be mediated by BCRP because hBCRP transports TGZS more efficiently than mBcrp.
The total clearance and hepatic concentration were not changed in Bcrp (–/–) mice, although biliary excretion is the predominant elimination pathway in wild-type mice. At steady state, the biliary excretion accounts for, at most, 30% of the total body clearance in Bcrp (–/–) mice, and the remaining fraction could be explained by other elimination mechanisms that were induced to compensate for the loss of biliary excretion. Urinary excretion could be an alternative elimination pathway of TGZS. However, the urinary excretion of TGZS was negligible in Bcrp (–/–) mice. Therefore, induction of hepatic metabolic enzymes is a likely mechanism. Currently, there is no information regarding the enzymes that are induced in Bcrp (–/–) mice, and further studies are necessary to identify them.
The effect of BCRP on the intestinal reabsorption was examined using everted ileum sacs. The mucosal efflux clearance (CLmucosal) of TGZS represents the intrinsic efflux ability of TGZS in the brush-border membrane of the intestinal epithelial cells, and the effect of BCRP on the mucosal excretion of TGZS can be measured by a comparison of CLmucosal between wild-type and Bcrp (–/–) mice. The CLmucosal of TGZS showed only a slight reduction in Bcrp (–/–) mice. This result suggests that BCRP plays only a limited role in preventing oral absorption of TGZS.

The effect of BCRP on the intestinal transport of TGZS in everted ileum sacs. a, the time courses of the mucosal efflux of TGZS. b, the tissue concentrations of TGZS after a 60-min incubation. c, the mucosal efflux clearances of TGZS. The data in wild-type mice are shown by closed circles or columns and those in Bcrp (–/–) mice by open circles or columns. All the data are represented by mean values ± S.E. of four everted sacs independently prepared from four mice. Asterisks represent statically significant differences between wild-type and Bcrp (–/–) mice; *, P < 0.05 and ***, P < 0.001.

Schematic representation of the molecular mechanism involved in the hepatic disposition of TGZS.
Figure 5 summarizes the molecular mechanism involved in the hepatic disposition of TGZS. TGZS is produced by SULT1A1 from TGZ and is excreted into the bile mainly by BCRP. TGZS excreted into the intestinal lumen undergoes reabsorption into the circulating blood (Kawai et al., 2000). SULT1A1, BCRP, and OATP1B1 are the important molecules controlling the hepatic disposition of TGZS. BCRP has some functional single nucleotide polymorphisms (SNP), such as C376T (Q126stop), C421A (Q141K), and G1322A (S441N). The C376T mutation introduces a stop codon, resulting in the production of truncated BCRP (Imai et al., 2002). The C421A allele is associated with a reduction in the protein level (Imai et al., 2002; Kondo et al., 2004; Kobayashi et al., 2005). The G1322A allele affects both the protein level and localization of BCRP (Kondo et al., 2004). Among these SNP, C421A exhibits the highest frequency (about 10 and 30% in Caucasian and Japanese, respectively) (Kobayashi et al., 2005). Clinical studies revealed that the plasma exposure of diflomotecan, topotecan, and rosuvastatin was higher in subjects carrying the C421A allele (Sparreboom et al., 2004, 2005; Zhang et al., 2006). These functional SNP of BCRP may increase the liver and/or plasma exposure of TGZS, affecting the susceptibility to TGZS if any induction of compensatory mechanisms, which were observed in Bcrp (–/–) mice but do not occur in humans. Besides BCRP, SULT1A1 and OATP1B1 also have functional SNP (Raftogianis et al., 1997; Nowell et al., 2002; Nishizato et al., 2003; Mwinyi et al., 2004; Wegman et al., 2005; Maeda et al., 2006). A combination of these functional SNP in BCRP, SULT1A1, and OATP1B1 may be involved in the idiosyncratic hepatotoxicity of TGZ.
In conclusion, our present study revealed that TGZS is a substrate of mBcrp and hBCRP and that the biliary excretion of TGZS is mainly mediated by BCRP in mice.
Acknowledgments
We thank Sankyo Co. Ltd. for supplying us with TGZ and TGZS, Dr. Kazuya Maeda and Soichiro Matsushima for providing MDCK cells expressing OATP1B1, and Dr. Alfred H. Schinkel (The Netherlands Cancer Institute, The Netherlands) for supplying Bcrp (–/–) mice.
Footnotes
-
This study was supported by Health and Labour Sciences Research Grants for Research on Regulatory Science of Pharmaceuticals and Medical Devices from Ministry of Health, Labour, and Welfare for the Research on Advanced Medical Technology.
-
Article, publication date, and citation information can be found at http://dmd.aspetjournals.org.
-
doi:10.1124/dmd.106.012567.
-
ABBREVIATIONS: TGZ, troglitazone; TGZS, troglitazone sulfate; BSEP, bile salt excrete pump; SULT, sulfotransferase; OATP, organic anion transporting polypeptide; MRP2/Mrp2, multidrug resistance-associated protein 2; BCRP/Bcrp, breast cancer resistance protein; ME3277, sodium hydrogen {4-[(4,5,6,7-tetrahydrothieno {3,2-c} pyridin-2-yl) carbonylamino] acetyl-o-phenylene} dioxydiacetate; MDCKII, Madin-Darby canine kidney II; GFP, green fluorescent protein; mBcrp, mouse Bcrp; hBCRP, human BCRP; PBS, phosphate-buffered saline; LC/MS, liquid chromatography/mass spectrometry; BSA-KRB, bovine serum albumin/Krebs-Ringer bicarbonate; SNP, single nucleotide polymorphism(s).
- Received August 27, 2006.
- Accepted November 1, 2006.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}