


Abstract
Apixaban, a potent and highly selective factor Xa inhibitor, is currently under development for treatment of arterial and venous thrombotic diseases. The distribution, metabolism, and elimination of [14C]apixaban were investigated in male, female, pregnant, and lactating rats after single oral doses. Tissue distribution of radioactivity in rats was measured using quantitative whole-body autoradiography. After a single oral administration, radioactivity distributed quickly in rats with Cmax at 1 h for most tissues. The elimination t1/2 of radioactivity in blood was 1.7 to 4.2 h. The blood area under the plasma concentration-time curve of radioactivity was similar between male and female rats and was slightly higher in pregnant rats and lower in lactating rats. The radioactivity concentration in tissues involved in elimination was greater than that in blood with the highest concentration in the gastrointestinal tract, liver, and urinary bladder/contents and lowest level in brains. In pregnant rats, the whole-body autoradiogram showed that low levels of radioactivity were present in fetal blood, liver, and kidney and were much lower than the radioactivity in the respective maternal organs. The fecal route was the major pathway (74% of dose), and the urinary route was the minor pathway (14%) for apixaban elimination. After single oral doses of [14C]apixaban to lactating rats, apixaban exhibited extensive lacteal excretion with apixaban as the major component. In summary, tissue distribution of apixaban in rats was extensive but with limited transfer to fetal and brain tissues and extensive secretion into rat milk with the parent drug as the major component. Milk excretion could account for 10% of apixaban dose, which was comparable to urinary elimination in rats. Tissue distribution and drug excretion of apixaban are consistent with those for a moderately permeable drug that is a substrate for P-glycoprotein and breast cancer resistance protein efflux transporters.
Introduction
Factor Xa is a key serine protease in the coagulation cascade and is a promising target enzyme for new therapeutic agents to treat and prevent arterial and venous thrombosis (Kaiser, 2002; Samama, 2002; Walenga et al., 2003). In particular, factor Xa plays a critical role in blood coagulation, serving as the juncture between the extrinsic (tissue factor-initiated) and intrinsic (surface activation and amplification) systems (Mann et al., 2003). Apixaban is an oral, potent, reversible, selective, and direct factor Xa inhibitor, which inhibits both free and prothrombinase-bound factor Xa activity and shows considerable efficacy in the prevention of arterial and venous thrombosis at doses that preserved hemostasis in rabbits (Pinto et al., 2007; Wong et al., 2008). Apixaban is also effective and safe for the prevention and treatment of venous thrombosis in humans (Lassen et al., 2007; Botticelli Investigators, 2008; APPRAISE Steering Committee and Investigators, 2009). Apixaban was well absorbed in rats, dogs, and humans (bioavailability of 34–80%, respectively). The mean volume distribution of apixaban was 0.31, 0.2 to 0.29, and 0.3 l/kg in rats, dogs, and humans, respectively. The systemic clearance of apixaban was low, representing <10, <3, and 5% of hepatic blood flows in rats, dogs, and humans, respectively (Shantsila and Lip, 2008). Apixaban was metabolized by multiple pathways in animals and humans (Zhang et al., 2009) and the fecal route was a major elimination pathway, accounting for >54% of dose in animals and >46% in humans. The urinary elimination accounted for <15% in animals and 25 to 28% of dose in humans (Zhang et al., 2009). In this study, the distribution, elimination, and milk excretion properties after single oral doses of [14C]apixaban in male, female, pregnant, and lactating rats were investigated.
Materials and Methods
Materials.
[14C]Apixaban (specific activity 20.1 μCi/mg and radiochemical purity >99.8%) was synthesized at Bristol-Myers Squibb (Princeton, NJ) (Zhang et al., 2009). All organic solvents and water were of HPLC grade.
Dose Preparation.
The oral dosing formulation was prepared on the day of dosing by addition of [14C]apixaban to a 0.5% Tween 80 in Labrafil (w/w) vehicle. For the tissue distribution study, the final drug concentration and radioactivity of [14C]apixaban in dosing solution were 1.0 mg/ml and 20 μCi/ml, respectively; For the milk excretion study, the final drug concentration and radioactivity of [14C]apixaban in dosing solution were 5.0 mg/ml and 20 μCi/ml, respectively. The concentration and homogeneity of [14C]apixaban were verified before and after dosing by counting triplicate aliquots of the formulation using liquid scintillation counting (LSC). The mean predose radioactivity concentration was used in calculation of the amount of radioactivity administered to each animal.
Animal Preparation and Dosing.
Before study initiation, the study protocol was approved by the institutional animal care and use committee. All animal housing and care conformed to the standards recommended by the Guide for the Care and Use of Laboratory Animals (Institute of Laboratory Animal Resources, 1996). Sprague-Dawley (SD) rats were purchased from Harlan (Indianapolis, IN) or Hilltop Laboratories (Scottdale, PA). Each animal was weighed, randomized, assigned a permanent identification number, and identified with a tail mark. During the acclimation period (at least 2 days before study initiation), the animals were housed in individual, suspended, stainless steel wire mesh cages, and food (Certified Rodent Diet 5002; PMI Nutrition International, St. Louis, MO) and water were provided ad libitum, except when animals were fasted overnight (at least 12 h) before and through 4 h after dose administration. The animal room was controlled to maintain a temperature of 75°F and 70% relative humidity with a 12-h light/dark cycle. The light cycles may have occasionally been interrupted to perform study procedures. Animals were placed in individual plastic shoebox cages with raised wire flooring and bedding and housed in these cages throughout the study period. The body weight of each rat was determined on the day before dosing. The doses administered were calculated on the basis of the body weight of each rat. The formulated [14C]apixaban was administered to fasted animals from each group by oral gavage using a syringe with a gavage needle to deliver a dose at a target dose level. The amount of dose administered to each rat was determined by the difference in weights of the loaded dose syringe and needle before dose administration and the emptied syringe and needle after dose administration.
Tissue distribution study.
Eight male SD rats (group 1, body weight of 225–252 g), eight female SD rats (group 2, body weight of 206–213 g), and six pregnant female SD rats (group 3, body weight of 270–319 g) were used for the tissue distribution study. Each rat received a single oral dose of [14C]apixaban at 5 mg/kg (100 μCi/kg). After dosing, rats were returned to their home cage and cage-side observations were performed on the day of dosing and at least daily for the remainder of the study. One male rat per time point from group 1 and one female rat per time point from group 2 were euthanized at 0.5, 1, 4, 8, 24, 72, 96, and 168 h postdose. One pregnant female rat was euthanized at 0.5, 1, 4, 8, 24, and 48 h. Blood samples (4–10 ml) from each rat were collected into tubes containing K3EDTA anticoagulant and were placed immediately on wet ice and then were centrifuged at 1300g for 10 min to obtain plasma and blood cells. Animals were euthanized, and each carcass was frozen in a hexane-dry ice bath for at least 15 min. All carcasses were stored at −20°C before preparation for tissue distribution by QWBA.
Milk excretion study.
Nineteen female SD rats were used for this study and each received a single oral dose of [14C]apixaban at 5 mg/kg (108 μCi/kg). Milk was collected from one rat predose and three rats per time point at 0.5, 1, 2, 6, 12, and 24 h postdose. Rats were given a subcutaneous injection (0.2 ml) of oxytocin 15 min before milk collection to stimulate lactation. Rats were anesthetized before the start of milk collection, and 1 ml of milk was collected from each rat using a specially constructed milking machine. The weight of each milk sample was recorded, and samples were placed immediately on wet ice or refrigerated until aliquoted for radioanalysis. After milk collection, rats were sacrificed by cardiac puncture under isoflurane anesthesia and 4- to 10-ml blood samples were collected into tubes containing K3EDTA anticoagulant. Blood samples were placed immediately on wet ice and then were centrifuged at 1300g for 10 min to obtain plasma.
Elimination study.
Three male SD rats (body weight approximately 300 g) were used for the mass balance study. Each rat received a single oral dose of [14C]apixaban at 30 mg/kg (150 μCi/kg). Urine and feces were collected from each rat over the time interval of 0 to 24, 24 to 48, 48 to 72, 72 to 96, 96 to 120, 120 to 144, and 144 to 168 h postdose.
Whole-Body Autoradiography.
QWBA assays were performed essentially as described previously (Solon et al., 2002). In brief, each frozen rat carcass was embedded in a 2% carboxymethylcellulose matrix with a microtome stage at −20°C. Three quality control standards of [14C]glucose at 0.05 μCi/g were placed into the frozen blocks before sectioning and were used for section thickness quality control. Whole-body sections at 40-μm thick were taken in the sagittal plane and captured on adhesive tape (Scotch Tape 8210; 3M Ltd., St. Paul, MN). Sections at various levels in the whole body were collected to include the major tissues, organs, and biological fluids; the whole-body sections were dried in the cryomicrotome at −20°C for at least 48 h. Once dried, a set of sections for each rat was mounted on a cardboard backing, covered with a thin plastic wrap, and exposed along with calibration standards of [14C]glucose at 10 different concentrations (0.001–6.5 μCi/g) to a 14C-sensitive phosphor imaging plate (Fuji Biomedical, Stamford, CT). The imaging plates and sections were placed in light-tight exposure cassettes and were kept in a copper-lined lead radiation safe chamber for a 4-day exposure at room temperature. After exposure, the imaging plates were scanned using the Typhoon 9410 image acquisition system (GE Healthcare, Little Chalfont, Buckinghamshire, UK), and the whole-body images were stored in a computer. Radioactivity concentration of tissues was quantified using MCID image analysis software (version 7.0; Imaging Research, Inc., St. Catherines, ON, Canada) based on the calibration standards of [14C]glucose. The concentrations of radioactivity were expressed as the microgram equivalents of apixaban per gram of sample. An upper and lower limit of quantification was applied to the data. The upper and lower limits of quantification were determined by using the radioactive concentration of the highest and lowest calibration standards divided by the specific activity of the test article in formulation.
Radioactivity Determination.
Radioactivity in samples of plasma, blood, milk, urine, or feces was determined using a Packard Tri-Carb model 2250CA LSC, and recovery of radioactivity in urine and feces was calculated. Fifty to 100 μl of each plasma, blood, milk, or urine sample was used for radioactivity determination in duplicate by adding 15 ml of Ecolite liquid scintillation cocktail and was counted for 10 min. Individual homogenized fecal samples (0.2 g each) were added with 1 ml of Soluene-350 and incubated overnight with gentle shaking in a 60°C water bath. After cooling, 0.2 ml of 30% hydrogen peroxide and 15 ml of Ecolite were added to each sample and mixed well, and the sample was then counted for 10 min in the LSC.
Metabolite Profile.
Metabolites in rat plasma, milk, urine, and fecal samples were profiled as described previously (Raghavan et al., 2009; Zhang et al., 2009). In brief, pooled plasma, milk, and feces samples were extracted in duplicate by addition of 4 ml of acetonitrile-methanol (1:1, v/v) to 1 ml of each sample, while the sample was mixed on a vortex mixer. After centrifugation at 2000g for 1 h, each supernatant fraction was removed and saved. The precipitate was resuspended in 2 ml of acetonitrile and 1 ml of methanol. After centrifugation of the mixture for 30 min at 2000g, the supernatant fraction was removed and combined with the first supernatant. The combined supernatant fraction was evaporated to dryness under nitrogen and reconstituted in 0.15 ml of acetonitrile and 0.05 ml of methanol. After centrifugation at 2000g for 5 min, a 100-μl portion of supernatant was injected into the HPLC system for metabolite profiling and identification. Pooled urine sample (1 ml) was centrifuged at 2000g for 5 min, and a 100-μl portion of supernatant was injected into the HPLC system for metabolite profiling and identification. The HPLC system was an Agilent 1100 series system equipped with two pumps, an autoinjector, a UV detector, and an ACE 3 C18 column (4.6 × 150 mm). The mobile phase consisted of two solvents: solvent A, 0.4% formic acid in water, pH 3.2; and solvent B, 100% acetonitrile. The gradient used was as follows: solvent B started at 5%; then linearly increased to 20% at 5 min, to 30% at 50 min, to 35% at 55 min, and to 90% at 65 min; was held at 90% for 2 min; and then decreased to 5% at 69 min. The HPLC effluent (0.7 ml/min) was collected into Deepwell LumaPlate-96 plates (PerkinElmer Life and Analytical Sciences, Waltham, MA) at 0.25-min intervals for 75 min with a Gilson model 204 fraction collector (Gilson, Inc., Middleton, WI). The plates were dried with a Savant Speed-Vac System (Global Medical Instrumentation, Inc., Ramsey, MN) and counted for 10 min/well with a TopCount analyzer (PerkinElmer Life and Analytical Sciences). Radioactivity profiles were prepared by plotting the resulting net counts per minute values versus HPLC time and radiochromatograms were reconstructed from the TopCount data using Microsoft Excel software.
Metabolite Identification.
Metabolites in rat plasma, milk, urine, and fecal samples were analyzed as described previously (Zhang et al., 2009). Liquid chromatography-tandem mass spectrometry analyses were performed on a LTQ mass spectrometer (Thermo Fisher Scientific, Waltham, MA) with an electrospray ionization probe and an Agilent 1100 series HPLC system equipped with two pumps, an autoinjector, and a UV detector (Agilent Technologies, Santa Clara, CA). The HPLC separation of the samples was performed using an ACE C18 column (3 μm, 4.6 × 150 mm). Samples were analyzed in the positive ionization mode, and the capillary temperature was set at 280°C. The flow rates of nitrogen gas, spray current, and voltages were adjusted to give maximum sensitivity for the apixaban. The HPLC mobile phases and running conditions were the same as those listed under Metabolite Profile.
Data Analysis.
Pharmacokinetic parameters in blood, plasma, and milk were calculated from the whole-body autoradiogram data or LSC data. These parameters included area under the concentration-time curve from time 0 to the last measurable time point (AUC0–t), and area under the concentration-time curve from 0 to infinity (AUC0–inf), the maximal concentration (Cmax), Tmax (the time to reach Cmax), and half-life time (t1/2). Pharmacokinetic parameters were calculated by using WinNonlin Professional Edition (version 4.1; Pharsight, Mountain View, CA).
Results
Tissue Distribution of Radioactivity.
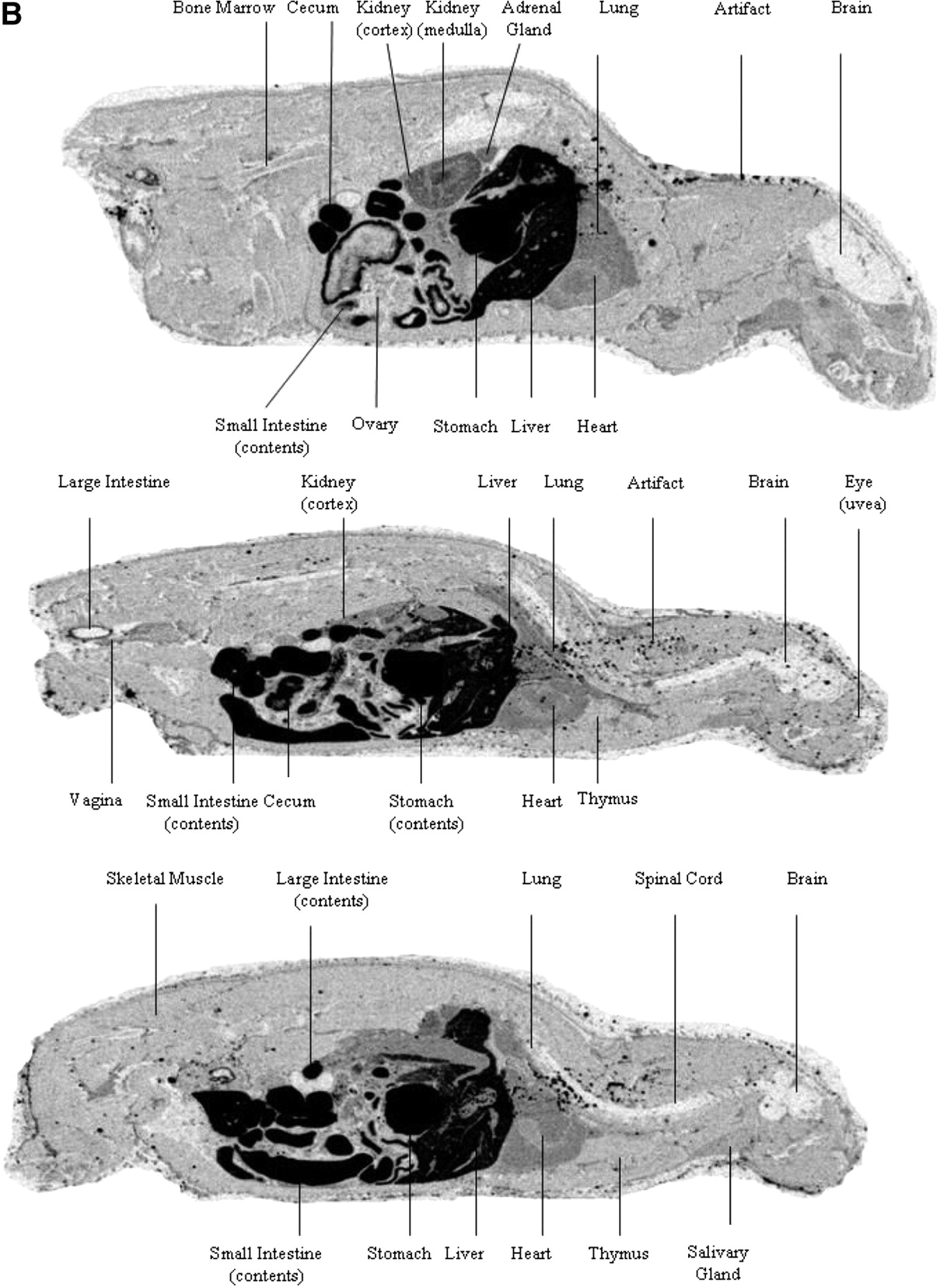
After single oral doses of [14C]apixaban (5 mg/kg) to rats, the distribution of radioactivity in rat tissues was determined using QWBA and the results are listed in Tables 1 to 3. As shown in Fig. 1, A to C, the distribution of [14C]apixaban-derived radioactivity was extensive in the tissues of male, female, and pregnant rats. The general trend of radioactivity concentration determined in rat tissues was slightly higher in pregnant rats than that in male and female rats. In all rats, the highest radioactivity appeared in the gastrointestinal tract, followed by liver, kidney, adrenal gland, blood, adipose, lung, heart, salivary gland, pancreas, thymus, muscle, and other tissues (Tables 1⇓–3; Fig. 1, A–C) and the lowest radioactivity appeared in brains. The Cmax of radioactivity in most tissues was reached at 1 h postdose. After 8 h postdose, radioactivity was eliminated quickly in kidney, lung, heart, spleen, and other tissues. At 24 h after dosing, nearly the entire administered radioactivity was eliminated from the rat body. No significant differences in tissue retention of [14C]apixaban were seen among the male, female, and pregnant rats, and radioactivity in all rat tissues was below the limit of quantitation or undetectable at 48 h postdose.
Tissue distribution of radioactivity in male rats after a single oral dose of [14C]apixaban at 5 mg/kg
Tissue distribution of radioactivity in female rats after a single oral dose of [14C]apixaban at 5 mg/kg
Tissue distribution of radioactivity in pregnant rats after a single oral dose of [14C]apixaban at 5 mg/kg



A, representative whole-body autoradiogram of radioactivity distribution in a male rat at 1 h after a single oral administration of [14C]apixaban (5 mg/kg). B, representative whole-body autoradiogram of radioactivity distribution in a female rat at 1 h after a single oral administration of [14C]apixaban (5 mg/kg). C, representative whole-body autoradiogram of radioactivity distribution in a pregnant rat at 1 h after a single oral administration of [14C]apixaban (5 mg/kg).
After a single oral dose of [14C]apixaban to pregnant rats, only low levels of radioactivity were detected in fetal tissues (Table 3; Fig. 1C). Fetal brains showed the lowest level of radioactivity. The Cmax of radioactivity in fetal tissues was reached at 4 h postdose; then the radioactivity concentrations in tissues of fetuses declined quickly and were below the limit of quantitation at 24 h postdose. At 48 h postdose, the overall radioactivity in maternal rats and fetuses was below the quantitation limit. The result also showed that radioactivity in amnion membrane was higher than that in other fetal tissues in all time points from 0.5 to 24 h (Fig. 1C).
Pharmacokinetics of Tissue Distribution.
After oral administration of [14C]apixaban to rats, the pharmacokinetic parameters (Tmax, Cmax, t1/2, and AUC) of radioactivity in blood were determined, and the results are presented in Table 4. The results showed that the Cmax of radioactivity in blood was reached at 0.5 to 1 h (Tmax) postdose. After the peak concentrations were achieved in blood (Cmax was 1180, 880, 1440, and 514 ng Eq/g for male, female, pregnant, and lactating rats, respectively), the blood radioactivity then declined in a log-linear manner until the end of the study at 168 h with a rapid elimination (t1/2 ranged from 1.7–2.9 h). The results showed that pharmacokinetic parameters were similar between male and female rats. However, the AUC value was higher in pregnant rats (7200 ng Eq · h/g) and lower in lactating rats (1940 ng Eq · h/g) than in male and female rats (4300 and 3780 ng Eq · h/g, respectively).
Pharmacokinetic parameters of radioactivity in blood and milk after a single oral dose of [14C]apixaban (5 mg/kg) to rats
Milk Excretion.
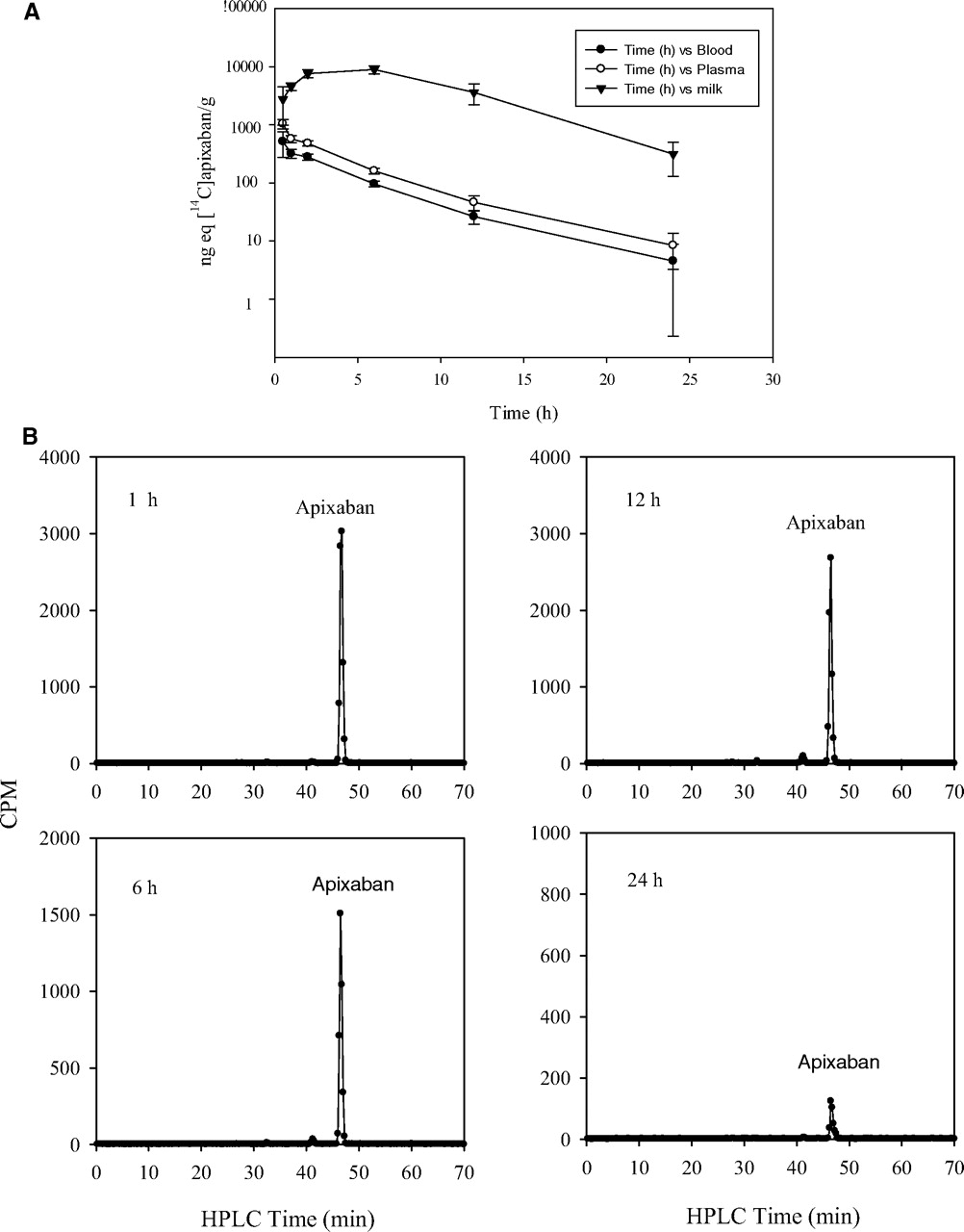
After a single oral dose of [14C]apixaban at 5 mg/kg (150 μCi/kg) to lactating rats, [14C]apixaban-derived radioactivity was extensively excreted in milk and was detected at all time points through 24 h postdose. The radioactivity concentration of apixaban-equivalent in milk at each time point was greater than that in blood or plasma. The Tmax value of radioactivity in milk (6 h) was later than that in plasma and blood (Table 4). The elimination t1/2 was similar between plasma and milk (Table 4). The milk/plasma concentration ratios ranged from 2.8 to 37. The milk AUC0–inf was approximately 30-fold greater than the plasma AUC0–inf (Table 4). The time-concentration profiles of radioactivity in plasma, blood, and milk are shown in Fig. 2A. Apixaban was the predominant component (>96%) in milk samples (Fig. 2B). The average body weight of female rats used in this study was 270 g, and the apixaban concentration in the collected milk was 2.75, 4.56, 7.59, 8.92, 3.61, and 0.31 μg/ml at 0.5, 1, 2, 6, 12, and 24 h, respectively. The time-averaged apixaban concentration in the 0 to 24 h milk was 4.6 μg/ml.

A, radioactivity profiles of blood, plasma, and milk at specified times after a single oral administration of [14C]apixaban (5 mg/kg) to rats. B, radioactivity profiles of rat milk samples at 1, 6, 12, and 24 h after a single oral administration of [14C]apixaban (5 mg/kg).
Routes of Elimination.
After single oral dose of [14C]apixaban, the average recovery of total radioactivity in rat urine and feces over the 0 to 168 h collection period was more than 89%. Fecal excretion accounted for approximately 74% (range from 68.6 to 77.6%) of radioactive dose. Approximately 14% of radioactive dose was recovered in urine.
Metabolic Profile and Identification.
Metabolites were profiled in plasma, milk, urine, and feces, and the prominent peaks were investigated on the basis of the radiochromatographic profiles with mass spectrometry. Mass spectra were compared with the synthesized standards of apixaban, O-demethyl apixaban, and previously identified metabolites (Zhang et al., 2009).
The plasma profiling showed that the parent compound was the major component (representing 97% of plasma radioactivity). Metabolites were trace level compared with the parent drug in the 1-h plasma sample, and metabolic profiles of the plasma samples at 4, 12, and 24 h were qualitatively similar to those of the 1-h plasma sample (data not shown).
Figure 2B shows the radioactivity profiles of milk samples at 1, 6, 12, and 24 h after single oral doses of [14C]apixaban to rats. Apixaban was the major component, representing >96% of sample radioactivity. The profiles were qualitatively similar among milk samples at all time points, and metabolites were minor compared with the parent drug.
The predominant radioactive peak in rat urine was apixaban (93%). The remaining radioactivity was distributed among three minor radioactive peaks, including M2 (O-demethyl apixaban, 2%), M4 (hydroxy apixaban, 2%), and M7 (3-hydroxy apixaban, 1.3%). The major radioactivity peak in feces was parent compound (83%). The minor metabolites in feces included M2 (13%), M4 (0.6%), and M7 (2.6%), similar to the metabolite profile reported previously (Zhang et al., 2009).
Discussion
The purpose of this study was to investigate the tissue distribution and elimination of [14C]apixaban in male, female, pregnant, and lactating rats after single oral doses. After single oral administration, absorption of apixaban was rapid in rats, reaching Cmax at 1 h in blood and most organs. The radioactivity in blood and most tissues declined quickly with no detectable radioactivity at 24 h postdose. The recovery of radioactivity averaged 74% in feces and only approximately 14% in urine, suggesting that fecal excretion was the major elimination route for apixaban in rats. Metabolite profiling showed that the parent drug was the major component in rat plasma, milk, urine, and feces with several minor metabolites including M2, M4, and M7 present in urine (accounted for approximately 5% of dose) and feces (accounted for approximately 17% dose). On the basis of these results and those reported previously (Zhang et al., 2009), tissue distribution and elimination of radiolabel largely reflects that of unchanged apixaban in rats.
The distribution of radioactivity of [14C]apixaban in rats was extensive, and the distribution patterns were similar among male, female, and pregnant rats with limited placenta-fetal transfer. These results are consistent with a high permeability of apixaban in a parallel artificial membrane permeability assay (data not shown), which would lead to passive diffusion across lipid membranes. During the experimental period, the highest radioactivity was observed in the gastrointestinal tract and liver, which was consistent with the oral route administration and fecal excretion as a major elimination pathway of apixaban in rats. Radioactivity concentrations were also higher in rat kidney and urinary bladder, consistent with renal excretion as an important elimination pathway for apixaban in rats. Autoradiograms showed that the radioactivity level was considerably lower in rat brain than in other well perfused organs (e.g., heart, lung, and muscle), suggesting that apixaban had limited penetration through the blood-brain barrier. Several mechanisms could play a role in this observation, including efflux transporters in the blood-brain barrier. Several efflux transporters such as P-glycoprotein (P-gp) and the breast cancer resistance protein (BCRP) present in the blood-brain barrier and prevent or reduce drug entry (Bart et al., 2000; Bendayan et al., 2002; Cooray et al., 2002; Demeule et al., 2002; Golden and Pollack, 2003; Cisternino et al., 2004). The interactions of apixaban with efflux transporters in the blood-brain barrier could be a mechanism for the low level of radioactivity in rat brain because apixaban was a substrate of P-gp and BCRP (D. Zhang, unpublished observations).
In pregnant rats, the peak level of radioactivity in fetal blood was approximately 35% of that in maternal blood, and the overall exposure was lower in fetal organs than in comparative organs in the mother (Table 3; Fig. 1C). Studies have showed that the placental membrane offered a protective barrier for the developing fetus by reducing the entry of drugs from mother to fetus (Syme et al., 2004). Efflux transporters including BCRP, P-gp, and multidrug resistance protein 2 (Mrp 2) can transport xenobiotics/drugs from the fetal compartment to the maternal circulation and protect the fetus from potential toxicity (Lankas et al., 1998; Jonker et al., 2000; Ceckova-Novotna et al., 2006). BCRP is the most abundant transporter expressed in the placenta (Maliepaard et al., 2001). In human placenta, the mRNA level of BCRP was found to be even 10 times greater than that of P-gp (Ceckova et al., 2006), and the mRNA expression in placenta was 100 times greater than that in heart, lung, muscle, kidney, spleen, thymus, and pancreas (Doyle et al., 1998). Therefore, it is possible that BCRP plays an important role in the limited transfer of apixaban to the fetus for maternally administered drugs.
Drug transfer into breast milk is determined by many factors such as ionization, plasma protein binding, molecular weight, lipophilicity of the drug, and drug pharmacokinetics in the mother. In vivo animal studies showed that the excretion of some drugs into rat milk was due to the active transport mechanism (McNamara et al., 1992, 1996; Gerk et al., 2001; Alcorn and McNamara 2002). Apixaban is a nonionizable molecule. Our results showed that apixaban was extensively secreted into milk after a single oral dose of [14C]apixaban to lactating rats. The average milk consumption is 5 ml/day for the first 5 days after birth (Romero et al., 1975). Ten baby rats would consume 50 ml of milk/day, which would represent approximately 10% of the dose (average milk concentration of apixaban × milk volumes per average apixaban dose). Milk secretion has not been recognized as an elimination pathway of a drug; however, this pathway is reasonable during the lactation period for any compound that shows significant milk secretion. The lowest blood concentrations and AUC values in the lactating rats compared with those in other groups of rats (Table 4) could be due to milk excretion as an additional clearance pathway. BCRP is strongly induced in the mammary gland of mice, cows, and humans during lactation and is responsible for the active secretion of clinically and toxicologically important substrates (Jonker et al., 2005). In comparison, other efflux transporters such as P-gp, Mrp1, and Mrp 2 were found to be absent from breast tissue in lactating mouse, suggesting that these efflux transporters may not be as important as BCRP in terms of lacteal secretion. The list of BCRP substrates has grown quite large in recent years (Polgar et al., 2008), suggesting that drug secretion into breast milk may occur more commonly than previously thought.
In summary, after oral administration of [14C]apixaban, the tissue distribution of apixaban was extensive in male, female, and pregnant rats, but with limited transfer to brain and fetal tissues. There was extensive secretion of apixaban into milk. The parent drug was the predominant component in rat plasma, milk, urine, and feces. Tissue distribution and drug excretion of apixaban are consistent with those for a moderately permeable drug that is a substrate for P-gp and BCRP efflux transporters.
Authorship Contributions
Participated in research design: Wang, He, Humphreys, and Zhang.
Conducted experiments: Wang and Zhang.
Contributed new reagents or analytic tools: Maxwell.
Performed data analysis: Wang, Grossman, Tremaine, Humphreys, and Zhang.
Wrote or contributed to the writing of the manuscript: Wang, Grossman, Tremaine, Humphreys, and Zhang.
Footnotes
This study was supported by Bristol-Myers Squibb and Pfizer. Parts of the experiments were conducted at Charles River Laboratories and Quest Pharmaceutical Services.
Article, publication date, and citation information can be found at http://dmd.aspetjournals.org.
doi:10.1124/dmd.110.036442.
-
ABBREVIATIONS:
- HPLC
- high-performance liquid chromatography
- LSC
- liquid scintillation counting
- SD
- Sprague-Dawley
- QWBA
- whole-body autoradiography
- AUC
- area under the plasma concentration-time curve
- P-gp
- P-glycoprotein
- BCRP
- breast cancer resistance protein
- Mrp
- multidrug resistance protein.
- Received September 22, 2010.
- Accepted November 8, 2010.
- Copyright © 2011 by The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}