Rhabdomyolysis after co-prescription of statin and fusidic acid
BMJ 2012; 345 doi: https://doi.org/10.1136/bmj.e6562 (Published 09 October 2012) Cite this as: BMJ 2012;345:e6562
- S Kearney, consultant neurologist1,
- A S Carr, specialist registrar in neurology1,
- J McConville, consultant neurologist2,
- M O McCarron, consultant neurologist3
- on behalf of the Northern Ireland Neurology Network
- 1Department of Neurology, Royal Victoria Hospital, Belfast Health and Social Care Trust, Northern Ireland
- 2Department of Neurology, Ulster Hospital, Dundonald, South Eastern Health and Social Care Trust, Northern Ireland.
- 3Department of Neurology, Altnagelvin Hospital, Derry, Western Health and Social Care Trust, BT47 6SB, Northern Ireland.
- Correspondence to: Seamus Kearney seamuskearney1{at}googlemail.com
Statins can cause a spectrum of muscle disorders ranging from an asymptomatic increase in serum creatine kinase concentration to life threatening rhabdomyolysis.1 The risk of statin myotoxicity is related to serum levels of the drug,2 and co-prescription with other drugs can influence statin levels and so increase risk.3 4 The British National Formulary emphasises muscle effects of statins and recommends avoidance of their concomitant use with fibrates, azole antifungals, antiretrovirals, and ciclosporin because of increased myopathy risk.5 An increased risk of myopathy with co-prescription of simvastatin and fusidic acid, and a possible increased myopathy risk with co-prescription of atorvastatin and fusidic acid are also identified, but avoidance of co-prescription was not explicitly recommended until 2012.5 This drug combination continues to be prescribed, with substantial associated morbidity and mortality.
We report eight cases of rhabdomyolysis apparently precipitated by fusidic acid in patients already taking statins. We highlight the potential seriousness of this interaction and continued co-prescription.
Case reports
Between 2006 and March 2012, eight patients with rhabdomyolysis attributed to co-prescription of a statin and fusidic acid were identified by the Northern Ireland neurology service. Northern Ireland has a population of approximately 1.7 million and is served by a “hub and spoke” neurology service from Belfast. We present clinical accounts of two representative cases, and table 1⇓ provides a summary of all the cases.
Cases of rhabdomyolysis associated with co-prescription of statin and fusidic acid identified by Northern Ireland neurology service during 2006–March 2012
Case 1
A 59 year old man with type 2 diabetes and ischaemic heart disease underwent coronary artery bypass grafting in July 2006. He had been taking atorvastatin 40 mg daily for over a year without adverse effect and had normal baseline renal fuction. He developed a meticillin resistant Staphylococcus aureus (MRSA) sternotomy wound infection and was treated with oral fusidic acid (500 mg three times daily for four weeks) and intravenous vancomycin (1 g twice daily for two weeks). Ten days after starting the antibiotics, he developed leg pain and weakness that progressed over two weeks until he became non-ambulant. Examination revealed global limb weakness. Serum creatine kinase was elevated at 137 272 IU/L, and myoglobinuria was detected. Atorvastatin was stopped, and he was rehydrated. His clinical condition improved, and within 14 days his serum creatine kinase levels had fallen to 182 IU/L. No other aetiology for rhabdomyolysis was found. Six months later, the patient’s mobility had returned to normal, he had full limb strength, and his serum creatine kinase level was normal (127 IU/L).
Case 2
A 73 year old woman with congenital absence of the right kidney, chronic kidney disease (estimated glomerular filtration rate 46 mL/min/1.73 m2), depression, previous MRSA infection, osteoarthritis, and hypercholesterolaemia had been taking simvastatin 40 mg daily for three years without incident. In January 2011 she was started empirically on oral fusidic acid (500 mg three times daily) by her general practitioner for a urinary tract infection (midstream specimen of urine subsequently proved negative). Two weeks later, she developed proximal muscle weakness, diffuse muscle pain, and dark urine. Her creatine kinase level was 9065 IU/L. On admission to hospital, her simvastatin and antibiotics were stopped. She was rehydrated. No other cause for rhabdomyolysis was found. She spent 10 days in intensive care but did not require haemodialysis. She subsequently made a good recovery: her creatine kinase level normalised, and she was independently mobile when reviewed three months later.
Cohort
In our cohort of eight patients the median age at development of rhabdomyolysis was 70 years (range 59–77), and six were men. Median creatine kinase peak was 26 579 IU/L (range 9065–137 272). Seven cases were associated with simvastatin or atorvastatin, with a median dose of 40 mg/day (20–60). One case was associated with rosuvastatin. Median duration of statin treatment before rhabdomyolysis was 28 months (1–72). Median duration of oral fusidic acid treatment before rhabdomyolysis was three weeks (2–5). No other concomitant drugs were deemed relevant. Four cases were MRSA positive, and four cases required intensive care. There were two deaths as a direct result of the rhabdomyolysis: both patients died in intensive care with multisystem failure despite full supportive care. Median duration of hospital stay in the surviving patients was 12.5 days (9–41), and median creatinine concentration on discharge was 66 umol/L (50–134). Only one patient (case 2) had longstanding renal impairment, and none has been re-challenged with a statin-fusidic acid combination. The patients’ characteristics are similar to those of 18 previously reported cases (table 2⇓).6 7 8 9 10 11 12 13 14 15 16 17.
Published cases of rhabdomyolysis associated with co-prescription of statin and fusidic acid
Discussion
To date, this is the largest published case series of rhabdomyolysis associated with co-prescription of statin and fusidic acid.6 7 In all eight cases, there was a clear temporal association between starting fusidic acid and onset of rhabdomyolysis in patients already taking atorvastatin, simvastatin, or rosuvastatin. Although causation cannot be definitively established from case reports, the proportional reporting ratio was 53.3 (95% confidence interval 26.2 to 109.9) in our population, suggesting that the risk of rhabdomyolysis was 50-fold higher when patients were exposed to the combination of fusidic acid and a statin compared with exposure to a statin alone.
Pharmocodynamic characteristics suggest an interaction may result in increased serum levels of statin and so increase the potential for myotoxicity. Fusidic acid and most statins are highly protein bound.3 18 Fusidic acid undergoes hepatic metabolism, including glucuronidation,18 which is important in statin excretion.19 It is suspected that fusidic acid metabolism is mediated by the cytochrome P450 enzyme pathway,8 9 particularly the 3A4 system, which is the predominant metabolic pathway for simvastatin and atorvastatin. Rosuvastatin undergoes only limited cytochrome P450 metabolism via the 2C9 pathway, and it is unknown if this is involved in fusidic acid metabolism. However, rosuvastatin has a relatively long half life and high bioavailability,19 which may have been contributory in the case we report (case 6). Rhabdomyolysis associated with co-prescription of rosuvastatin and fusidic acid has not been previously reported.
We reviewed regional prescription data for Northern Ireland from 2008 to 2011.20 About 250 patients were co-prescribed a statin and fusidic acid for every 12 month period, with no change in rate over time (fig 1⇓). Assuming that the eight described cases represent all rhabdomyolysis caused by co-prescription of statin and fusidic acid in Northern Ireland over six years, this equates to a 1:188 risk of rhabdomyolysis requiring hospital admission and a 1:750 risk of death in patients receiving this combination of drugs. Although the small numbers of patients prompt caution in interpreting these risk estimates, statin prescription is common and increasing (fig 2⇓). The prevalence of prescription of any statin in January 2011 was 12.6 (95% confidence interval 12.5 to 12.6) per 100 people. This reaches 48.9 (48.8 to 49.0) per 100 people in those aged over 50 years. Together simvastatin and atorvastatin make up 80.4% of all statin prescriptions. Despite clinical and pharmacological data to advocate avoidance of statin-fusidic acid co-prescription, it continues and has the potential to increase. Of the available statins in the UK, pravastatin has comparatively lower protein binding and is less reliant on hepatic cytochrome metabolism, as it undergoes extensive gastric chemical degradation.21 Although our data alone cannot be interpreted as showing less myotoxicity from pravastatin when prescribed with fusidic acid, the absence of any such cases in the literature (n=26) suggests that there may be less risk with pravastatin.

Fig 1 Number of fusidic acid and statin co-prescriptions in Northern Ireland from 2008 to 2011 by 6 month intervals
{kind=link}
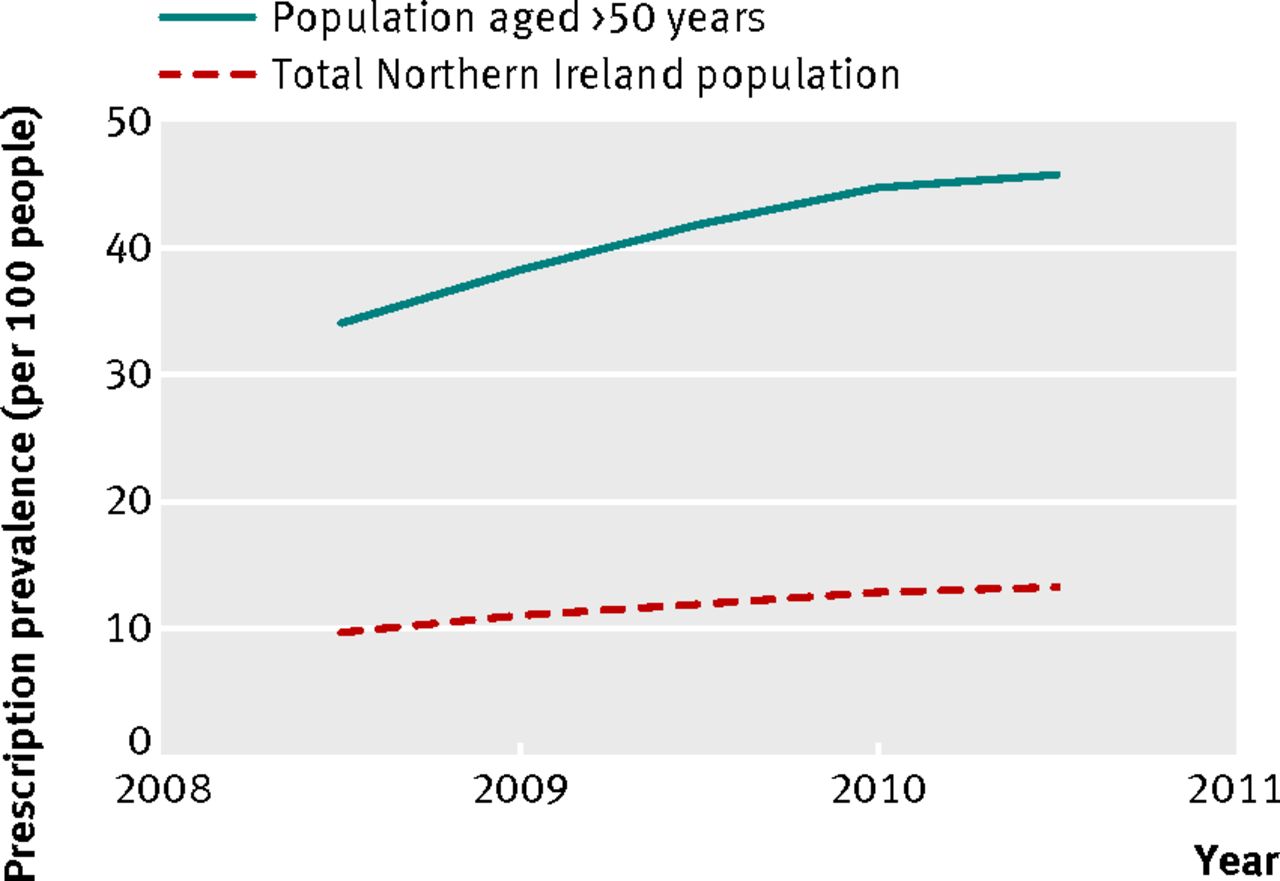
Fig 2 Prevalence of statin prescription in Northern Ireland from 2008 to 2011 by 6 month intervals
{kind=link}
Conclusion
This case series highlights important morbidity and mortality from a possible association between rhabdomyolysis and co-prescription of certain statins and fusidic acid. Convincing evidence exists for an interaction between these drugs. Given the increasing prevalence of statin use, including non-prescription availability, there is a high potential for frequent co-prescription. Our regional prescription data indicate nearly a third of patients treated with fusidic acid have concomitant statin prescription. In patients requiring both treatments, a possible solution is short term statin withdrawal, but this must be balanced against the risk of an adverse outcome from withdrawal, particularly in patients with acute coronary syndrome, ischaemic stroke, or after major vascular surgery.22 In the absence of demonstrable safety from other statins, we recommend better vigilance among clinicians to avoid co-prescription of statins and fusidic acid.
Notes
Cite this as: BMJ 2012;345:e6562
Footnotes
Contributors: All the authors made substantial contributions to conception and design of the study, analysis and interpretation of data, drafting and revising the manuscript for important intellectual content, and approval of the final version to be published. Raeburn Forbes, John Craig, Orla Gray, Cathy Jack, Tom Trinick, Brian Herron, and Gavin McDonnell, all members of the Northern Ireland Neurology Network, helped revise the manuscript for important intellectual content and approved the final version to be published. MOMcC is the guarantor of the paper.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent obtained.