


Abstract
Epacadostat (EPAC) is an indoleamine 2,3-dioxygenase 1 (IDO1) inhibitor that has been examined in multiple clinical trials. The substrate for IDO1 is tryptophan and there is a theoretical concern that inhibition of IDO1 may increase the concentrations of tryptophan and subsequently serotonin, potentially leading to serotonin syndrome (SS). The objective of this study was to evaluate the effect of EPAC, either alone or with linezolid, a monoamine oxidase inhibitor (MAOI), on brain extracellular fluid (ECF) concentrations of serotonin in rats, using microdialysis. While fluoxetine, a selective serotonin reuptake inhibitor, increased the serotonin ECF concentration by 2-fold, the combination of fluoxetine with linezolid (a positive control used in the study) resulted in a 9-fold increase. Neither EPAC monotherapy nor combination with linezolid had any effect on serotonin concentration. In addition, EPAC was shown to have poor penetration across the rat blood-brain barrier. Across multiple phase I/II clinical studies with EPAC, four SS-like episodes were observed out of 2490 subjects, but none of the incidences were confirmed as a true case of SS. These data suggest that EPAC is unlikely to cause SS following either monotherapy or in combination with MAOIs. Thus, the exclusion of MAOI from clinical studies with EPAC has been lifted.
Introduction
Serotonin syndrome (SS) is an adverse, toxic drug reaction caused by excessive serotonergic activity attributable to increased serotonin concentrations in the central nervous system (CNS), and is potentially life threatening (Bijl, 2004). Given the importance of serotonin in the CNS, the synthesis, transport, as well as metabolism of this neurotransmitter is well regulated by a mechanism involving a bidirectional communication system between the CNS and the gastrointestinal tract (O’Mahony et al., 2015). Serotonin is synthesized from the essential amino acid tryptophan through supplementation in the diet. Tryptophan is first converted to 5-hydroxytryptophan and then to serotonin. This process can take place both in the peripheral tissues and also in the brain. The majority of serotonin is located in the gut; however, it does not cross the blood-brain barrier (BBB). Instead, serotonin in the brain is synthesized from circulating tryptophan, which can cross the BBB via large neutral amino acid transporters (Wurtman et al., 1980). Thus, a drug that increases tryptophan either locally in the CNS or systemically could potentially impact serotonin levels in the brain (Wurtman et al., 1980).
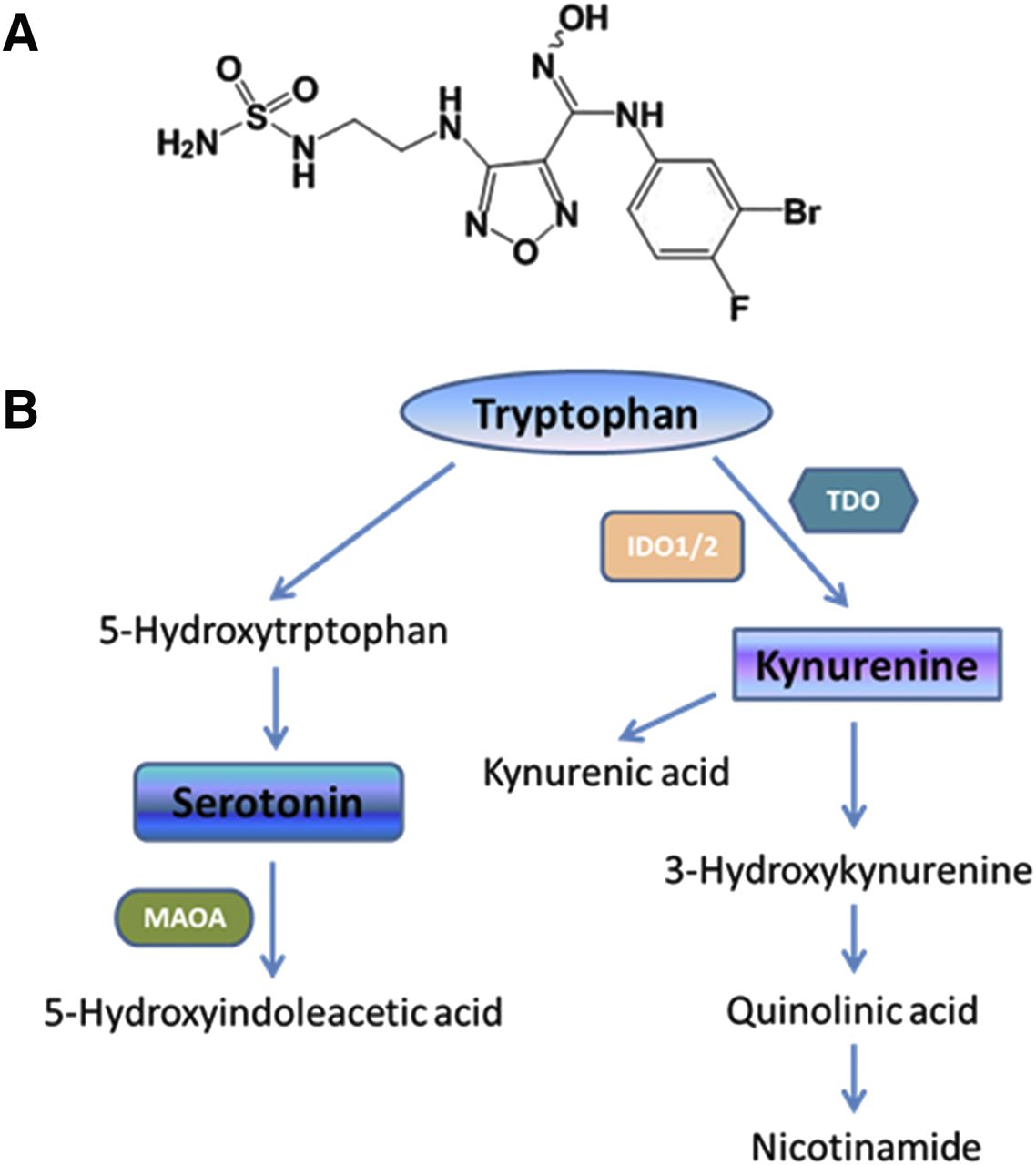
Tryptophan has dual metabolic pathways, with the kynurenine pathway accounting for approximately 95% and the serotonin pathway accounting for 5% of tryptophan catabolism (Prendergast et al., 2017). Epacadostat (EPAC) (Fig. 1A) is an inhibitor of the enzyme indoleamine 2,3-dioxygenase 1 (IDO1) (Liu et al., 2010; Yue et al., 2017), which has been examined in multiple clinical trials in combination with checkpoint modulators for immune-oncology diseases. IDO1 is a heme-containing enzyme that acts as the rate-limiting step in the breakdown of tryptophan along the kynurenine pathways (Oxenkrug, 2010) (Fig. 2). Therefore, a theoretical concern is raised that inhibition of IDO1 may increase the concentrations of serotonin in the brain by affecting the catabolic pathway of tryptophan either systemically or locally in the brain. Given the potential severity of serotonin toxicity clinically, several studies were employed. The goals of these investigations were to 1) determine whether EPAC can cross the rat BBB to have a local effect on the tryptophan metabolism; 2) examine whether oral administration of EPAC can increase brain serotonin levels in rats using microdialysis model; and 3) review the incidence of SS in patients given EPAC.

(A) Structure of EPAC (molecular weight = 437 g/mol). (B) Tryptophan metabolism pathway. Indoleamine 2,3-dioxygenase (IDO) is the first and rate-limiting catabolic enzyme in the degradation of the essential amino acid tryptophan along the kynurenine and serotonin pathways. The kynurenine pathway accounts for approximately 95% and the serotonin pathway accounts for 5% of tryptophan catabolism. In addition to IDO, tryptophan 2,3-dioxygenase (TDO) is also responsible for the conversion from tryptophan to kynurenine. IDO1 is expressed throughout the body and is overexpressed in multiple tumor types. IDO2 is similar to IDO1 by 41% at the amino acid level. However, its role in cancer is unclear. TDO is predominantly expressed in the liver and is responsible for the homeostasis of tryptophan levels in the body (Yue et al., 2017).

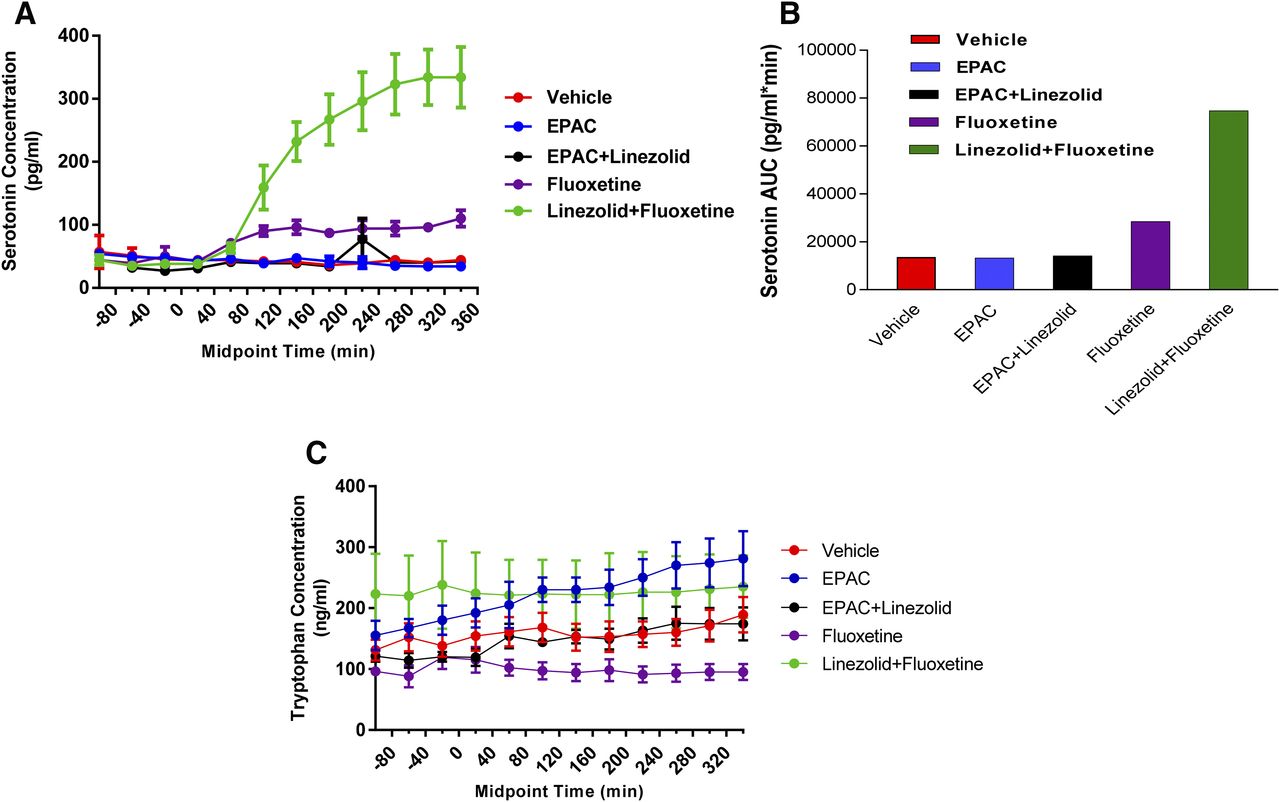
Serotonin, tryptophan, and kynurenine concentrations in rats following microdialysis studies. (A) Serotonin concentration vs. mid-time points following treatment with various test compounds. Data are presented as concentrations of serotonin at various sample-collecting time points vs. mid-time points. The results are expressed as the mean ± S.E.M. for three to four rats. (B) The area under the curve (AUC) for the concentration of serotonin following the treatment with vehicle, EPAC alone, EPAC plus linezolid, fluoxetine alone, or fluoxetine plus linezolid. The mean serotonin concentration-time data shown in (A) were used to determine the AUC values by standard noncompartmental methods using Phoenix WinNonlin (version 6.4.0; Pharsight Corporation, Mountain View, CA). (C) Tryptophan concentrations vs. mid-time points following treatment with vehicle, EPAC alone, EPAC plus linezolid, fluoxetine alone, or fluoxetine plus linezolid. Data are presented as concentrations of tryptophan at various sample-collecting time points vs. mid-time points. The results are expressed as mean ± S.E.M. for three to four rats.
While SS typically occurs following administration of two or more drugs that enhance serotonin concentrations, it can be induced by an overdose of a single agent (Boyer and Shannon, 2005). Therefore, single agents and combinations were used in these studies to demonstrate SS in this rat microdialysis model. Linezolid was the first synthetic oxazolidinone antimicrobial agent proven to be effective against nosocomial and community-acquired pneumonias and skin infections (Taylor et al., 2006). Linezolid inhibits monoamine oxidase A, which is responsible for the metabolism of serotonin in the brain. High concentrations of serotonin can build up in the brain following monoamine oxidase inhibitor dosing, especially when combined with other agents such as fluoxetine, which thus could increase intracerebral serotonin concentrations and cause toxicity (Patel and Galarneau, 2016). Fluoxetine is a selective serotonin reuptake inhibitor (SSRI), which by definition inhibits the reuptake of the extracellular serotonin by the presynaptic neurons, resulting in accumulation of serotonin within the presynaptic cleft (Cooper and Sejnowski, 2013). Both fluoxetine and its metabolite norfluoxetine have longer half-lives than other SSRIs, which is problematic from a drug interaction standpoint since it can precipitate SS even if discontinued as early as 5 weeks prior to another serotonergic agent being introduced (Boyer and Shannon, 2005; Patel and Galarneau, 2016).
In the current study, the effect of EPAC, either alone or when coadministrated with linezolid, on brain extracellular fluid (ECF) concentrations of serotonin in rats, using microdialysis, was determined. Linezolid in combination with fluoxetine was used as a positive control. In addition, the concentration of tryptophan in both plasma and brain ECF was also determined. In a separate experiment, brain uptake of EPAC in rats was evaluated to better understand the CNS distribution potential of EPAC. Our clinical data generated from 2490 subjects among multiple phase I/II studies were also collected to assess for any adverse events, including symptoms of SS.
Materials and Methods
Materials
Epacadostat was synthesized by Adesis (New Castle, DE). Linezolid was purchased from Cayman Chemical Company (Ann Arbor, MI), while fluoxetine was purchased from Sigma-Aldrich (St. Louis, MO). All other chemicals were purchased commercially and were either reagent or USP grade.
All animal use procedures conformed to the ethical standards. The studies were conducted in accordance with the principles and guidelines of the Institutional Animal Care and Use Committees (https://olaw.nih.gov/resources/tutorial/iacuc.htm) and of the Canadian Council on Animal Care for the care and use of laboratory animals (https://www.ccac.ca/).
Brain Uptake Studies in Rats
Male Sprague-Dawley rats (N = 4; Charles River Laboratory, Inc., Raleigh, NC), 8–10 weeks of age, were given EPAC via intravenous infusion after an intravenous bolus dose to rapidly attain steady state. Doses were selected to target a steady-state plasma concentration of ∼1 µM, which is relevant to a dose of 100 mg twice daily in clinic in the majority of the combination therapies. The intravenous bolus and infusion doses were 2 and 2 mg/kg per hour, respectively. EPAC was formulated in 5% dimethylacetamide in saline. The whole brain, cerebrospinal fluid (CSF), and a terminal blood sample were collected at 4 hours postdose. Blood samples were centrifuged to obtain plasma, CSF samples were diluted 2-fold in plasma to minimize adsorption, and the brain tissue was homogenized with water/acetonitrile/formic acid (95/5/0.1, v/v/v). All samples (plasma, CSF, and brain homogenate) were extracted with five volumes of acetonitrile/methanol (90/10, v/v) mixture. Concentration of EPAC in plasma, CSF, and brain were determined by liquid chromatography–tandem mass spectrometry using Turbo Spray ionization with a positive interface on a Sciex API-4000 (Applied Biosystems/MDS SCIEX, Concord, ON, Canada) and multiple reactions monitoring.
Microdialysis Studies in Rats and Data Analysis
Microdialysis Study.
The microdialysis studies in rats were conducted by Intervivo Solutions (Toronto, ON) and detailed information on the experimental setup, sampling, and quantitative determination of neurochemical analytes can be found elsewhere (Cudjoe et al., 2013). Briefly, male Sprague-Dawley rats were divided into four correspondent groups with four rats in each group. Rats were given either EPAC (25 mg/kg, by mouth) alone, linezolid (100 mg/kg, by mouth) with EPAC (25 mg/kg, by mouth), fluoxetine (10 mg/kg, i.p.) alone, or a combination of linezolid (100 mg/kg, by mouth) plus fluoxetine (10 mg/kg, i.p.). All formulations by mouth were prepared in 0.5% methylcellulose while fluoxetine was formulated in 0.9% sodium chloride solution. A microdialysis probe was implanted into the right striatum and a catheter was placed in the femoral artery of each rat. The microdialysis probe was perfused at 1 μl/min with artificial CSF and dialysate was collected over 40-minute intervals. Dialysate samples were collected prior to dosing (three baseline samples) and over 6 hours after the dose. Plasma concentrations of tryptophan in the vehicle and EPAC (25 mg/kg, by mouth) treatment groups were determine by liquid chromatography–tandem mass spectrometry. Liquid chromatography–tandem mass spectrometry methods were also used to quantify tryptophan, serotonin, and kynurenine in dialysate samples. Concentrations of each analyte determined in the dialysate samples collected following dosing were compared with those collected at baseline. Since the probes were perfused at a constant flow rate, the relative recovery of the analytes from the microdialysis system (tubing and probe) was assumed to be constant over the course of the experiment; therefore, the relative recovery was not independently evaluated. Mean dialysate concentrations of the analytes at each time interval following dosing were compared with the mean of the baseline concentrations for each individual animal. Data are presented as mean concentrations of each analyte over a series of sample-collecting time points. The results are expressed as the mean ± S.E.M. from three to four rats.
Clinical Study Design
Multiple clinical phase I/II studies for EPAC were conducted in subjects with advanced or metastatic cancers either as monotherapy or in combination with anti-PD-1 inhibitors (pembrolizumab or nivolumab), anti-PD-L1 inhibitors (atezolizumab or durvalumab), JAK inhibitors (itacitanib), anti-CTLA-4 (ipilimumab), and chemotherapy. These studies were conducted in full accordance with the Declaration of Helsinki; the Good Clinical Practice guidelines as required by and described in 21 Code of Federal Regulations parts 50, 54, 56, 312 subpart D, and 314 (https://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E6/E6_R1_Guideline.pdf). All of these studies were reviewed and approved by local or central ethics committees. In total, 2490 male and female subjects were included in these studies with twice daily doses of EPAC ranging from 25 to 700 mg at each dose. Subjects were excluded from EPAC clinical trials based on the following criteria: 1) a history of SS was reported after receiving serotonergic drugs; 2) a monoamine oxidase inhibitor (MAOI) was given within 21 days prior to enrollment and/or randomization; or 3) one of these prohibited medications was anticipated to be given during the treatment phase. Of note, the use of an SSRI was not prohibited and 188 subjects across these studies had taken an SSRI while being treated with EPAC either alone or in combination with another anticancer therapy. All subjects enrolled in clinical studies were provided a SS information card listing signs and symptoms of SS. This information card instructed participants to seek immediate medical care if any of the listed symptoms were observed. In the event that nonserious SS was reported, it would be considered as an event of clinical interest, which was required to be reported to the sponsor within five calendar days of awareness of the event. If the symptoms of SS met serious criteria, then reporting to the sponsor was required within 24 hours of awareness of the event. In addition, all subjects were assessed each cycle of treatment for any adverse events (including symptoms of SS) that occurred.
Results and Discussion
Serotonin is synthesized from essential amino acid tryptophan (Fig. 1B) in the brain and other peripheral tissues (Wurtman et al., 1980; Mbongue et al., 2015; O’Mahony et al., 2015). The central effects of serotonin are thought to include modulation of mood, the sleep-wake cycle, hormone secretion, sexual behavior, and thermoregulation (Bijl, 2004). Serotonin syndrome is believed to be caused by increased serotonin at the intrasynaptic cleft as the result of the pharmacological effect of a drug or a combination of drugs that modulate intracerebral serotonin concentrations (Bijl, 2004; Boyer and Shannon, 2005; Cooper and Sejnowski, 2013). There are various mechanisms by which drugs could potentially produce SS via their functions in serotonin clearance. Examples of those drugs include, but are not limited to, SSRIs and MAOIs. The former inhibit serotonin reuptake into presynaptic neurons, while the latter prevent the breakdown of serotonin (Cooper and Sejnowski, 2013).
EPAC is an inhibitor of the enzyme indoleamine IDO1. IDO1 is one of the key enzymes involved in the kynurenine metabolism pathway (Fig. 1B) (Mbongue et al., 2015). It is known that increasing the synthesis of serotonin by elevations in L-tryptophan can potentially lead to SS (Wurtman et al., 1980; Esteban et al., 2004). Its manifestation may be the result of the elevation of the tryptophan concentrations either through systemic circulation or via local effect at the synaptic cleft since serotonin does not cross the BBB. Therefore, it is possible that inhibition of IDO1 could precipitate a SS through alterations in the concentrations of tryptophan, and in turn serotonin. Animal models of SS can be helpful in identifying drugs and drug combinations that have the potential to induce SS in humans (Haberzettl et al., 2013), in addition to uncovering the mechanism behind the development of SS. The effects of a single dose of SSRI on serotonin concentrations using in vivo microdialysis techniques have been studied in rats. Fluoxetine (either through subcutaneous or intraperitoneal injection) augmented the serotonin concentrations by 110%–300% in the rat frontal cortex (Gobert et al., 1997; Koch et al., 2002; Cooper and Sejnowski, 2013). In this current rat microdialysis study, a moderate increase of up to 2-fold in ECF serotonin concentrations was demonstrated at approximately 120 minutes following treatment with fluoxetine (Fig. 2A). In addition, the 2-fold increase in serotonin concentrations was maintained during the treatment period, which is consistent with reported observation and the long half-life of fluoxetine. Some of the reversible inhibitors of monoamine oxidase A, such as linezolid, cannot produce SS when taken alone, even as an overdose (Lawrence et al., 2006). However, the concomitant administration of linezolid and a SSRI, such as fluoxetine, can boost the serotonin concentrations in the synaptic cleft, and therefore can augment the SS (Patel and Galarneau, 2016). In the current study, coadministration with fluoxetine resulted in a time-dependent increase in serotonin ECF concentrations in rats with a pronounced (9-fold) elevation being observed at approximately 300 minutes post-treatment (Fig. 2A).
The effect of EPAC on the ECF serotonin concentration levels was also determined in this study using microdialysis in freely moving conscious rats. Following a 25 mg/kg oral dose of EPAC (a dose that is equivalent to the 200–300 mg twice daily clinical dose), the average serotonin concentrations in brain ECF remained unchanged throughout the 360-minute treatment time period (Fig. 2A). Similar effects were also observed with coadministration of EPAC and linezolid, in that brain ECF serotonin concentrations were comparable to those in both the EPAC monotherapy and vehicle control groups (Fig. 2A).
To have a more direct comparison on the serotonin concentrations following each treatment option, the area under the curve values of serotonin collected during the −100 to 360 minute pre- and post-treatment periods were calculated (Fig. 2B). The values of the area under the curve of serotonin were comparable among the vehicle, EPAC, and combination of EPAC with linezolid groups. However, these values increased 2.1- and 5.5-fold to that of the vehicle group in the fluoxetine alone and the fluoxetine and linezolid cotreated groups, respectively (Fig. 2B). The present findings are in good agreement with literature published reports indicating that either SSRI alone or the combination with MAOI could cause SS. In addition, these data also suggested that the SS is unlikely following the treatment with EPAC, an IDO1 inhibitor, either as a single agent or combination treatment with MAOIs, such as linezolid.
Adequate brain uptake of the perpetrating agent is an expected requirement for modulation of intracerebral serotonin concentrations. Indeed, linezolid has shown good CNS penetration and is a promising candidate for treatment of CNS infections (Villani et al., 2002). In the supporting study, the brain penetration potential of EPAC was determined in rats following intravenous dosing. At steady state (4 hours postdose), the mean brain homogenate concentration of EPAC was 15% of the average plasma concentration of 0.851 µM (Table 1). Moreover, the CSF concentrations of EPAC were below the quantification limit of 0.004 µM, and therefore well below the corresponding free plasma concentration at steady state. These results support minimal brain penetration of EPAC in rats, which is in good agreement with a recent publication demonstrating the low brain penetration potential of EPAC in C57BL/6 mice following a 50 mg/kg oral dose with a correspondent plasma concentration close to 30 µM (Ladomersky et al., 2018). The restricted BBB penetration of EPAC may be due in part to efflux by both P-glycoprotein and/or breast cancer resistance protein (Zhang et al., 2017), two major efflux transporters expressed in the brain microvessel endothelial cells lining the BBB (Giacomini et al., 2010). The poor brain uptake for EPAC suggests that the potential for IDO1 inhibitory activity in the brain following EPAC oral dosing is limited.
Brain, CSF, and plasma concentrations of EPAC in rats following intravenous infusion for 4 h (N = 4)
As shown in Fig. 2A, treatment with fluoxetine alone or in combination with linezolid significantly increased the brain ECF serotonin concentrations in rats. The impact of these treatments on the brain ECF concentrations of tryptophan was also determined. Although there were large variations in the baseline concentrations of tryptophan between the two treatment groups, treatment with either fluoxetine alone or the combination of fluoxetine and linezolid did not have any significant effect on the brain ECF concentrations of tryptophan (Fig. 2C) in rats. The minimum impact on the ECF concentrations of tryptophan despite a drastic effect on the serotonin concentrations may be partially explained by the fact that these two compounds do not have a direct effect on the kynurenine pathway, which accounts for approximately 95% of tryptophan catabolism (Prendergast et al., 2017). In addition, this observation may also be due in part to the fact that both fluoxetine and linezolid have the brain penetration potential. Therefore, their impact on the local pool of serotonin in brain ECF is significant via interacting directly with the serotonin reuptake pathway (fluoxetine) or the serotonin metabolism pathway (linezolid) in the presynaptic cleft.
The ECF concentrations of tryptophan were also determined following treatment with either EPAC alone or in combination with linezolid. The tryptophan ECF concentrations did not change significantly following treatment with the combination of EPAC plus linezolid (Fig. 2C). Following administration of EPAC alone, there was a trend toward an increase in tryptophan concentrations in brain ECF; however, the changes were well within the normal range for tryptophan across studies. The lack of indoleamine 2,3-dioxygenase inhibitory effect in rat brain is likely a result of poor brain uptake of EPAC. Approximately 95% of the tryptophan metabolism pathway is through the kynurenine catabolic route (Prendergast et al., 2017); therefore, inhibition of IDO1 may have an impact on the tryptophan concentration systemically. In addition, since circulating tryptophan can cross the BBB (Wurtman et al., 1980), the plasma concentrations of tryptophan were determined in the EPAC alone and vehicle groups. Although the tryptophan concentration at 6 hours postdose with 25 mg/kg EPAC (220 ± 170 µM) was greater than that of the vehicle-treated group (157 ± 30 µM), these values were not statistically significantly different from each other, suggesting a minimal impact of EPAC treatment on systemic concentration of tryptophan.
The effect of EPAC (an IDO1 inhibitor that inhibits the conversion from tryptophan to kynurenine) on brain ECF concentrations of serotonin was minimal in rats using the microdialysis method. In addition, codosing of linezolid in the treatment did not have a significant impact on the serotonin concentration. In contrast, either fluoxetine alone or the combination with linezolid significantly increased the local pool of serotonin in the brain ECF of rats. The lack of effect on the serotonin ECF concentrations by EPAC may be partially explained by the fact that it has minimal penetration of the BBB. Furthermore, the fact that the concentration of circulating tryptophan following EPAC treatment was not statistically significantly different from the vehicle treatment group suggested that the impact of EPAC treatment on the circulating tryptophan, and consequently on the brain concentration of serotonin, is minimal.
Across the EPAC monotherapy and combination therapy clinical studies, subjects were closely monitored for clinical symptoms of SS. Only four cases of suspected SS have been reported among those 2490 subjects (six studies of EPAC monotherapy and 22 studies of EPAC in combination with other agents). The first case was a subject in the ECHO 202 Keynote-037/ECHO-202: Clinicaltrials.gov Identifier NCT02178722. (https://clinicaltrials.gov/ct2/show/NCT02178722?term=ECHO+202&rank=1) study that was testing the combination of EPAC with pembrolizumab in advanced or metastatic cancers. The subject reported chills, increased blood pressure, and increased temperature [all common terminology criteria for adverse events (CTCAE) grade 1] on day 1 of treatment. These events resolved within 1 week while dosing was stopped. The subject was treated with lorazepam and toradol. The subject was taking escitalopram, an SSRI. While he experienced mild symptoms, the full constellation of SS was not observed nor could it be ruled out. The SSRI was discontinued and the subject was able to restart EPAC about 1 week later at the same dose level of 100 mg twice a day without further incidents. The second case was a subject treated in the ECHO 203 (ClinicalTrials.gov Identifier NCT02318277. https://clinicaltrials.gov/show/NCT02318277) study that was testing the combination of EPAC with durvalumab in advanced solid tumors. The subject reported tremors (CTCAE grade 1) and agitation (CTCAE grade 2) on study day 47 and was assessed for SS on study day 56. The subject was not on an SSRI but was on a medication for anxiety (Alprazolam). The full constellation of SS was not observed nor could it be ruled out. The events resolved and the dosing with EPAC was interrupted for 1 week. Retreatment started with a lower oral dose of EPAC of 50 mg twice a day from 75 mg twice a day on study day 58 without further incidents. The third case involved a subject treated in ECHO 306 (Keynote-715-05/ECHO-306-05. ClinicalTrials.gov Identifier: NCT03322566. https://clinicaltrials.gov/show/NCT03322566.), a combination study with pembrolizumab and 100 mg EPAC twice a day in nonsmall cell lung cancer, taking granisetron, an antiemetic. The subject reported chills, fever, tremors, tachycardia, and hyper-reflexia (CTCAE grade 1) on day 16. The recovery was confirmed as the symptoms resolved after treatment with cyproheptadine. The subject stopped epacadostat but continued on pembrolizumab and pemetrexed. The fourth case was a subject on study ONC-DPX-Survivac-06, a combination of EPAC 300 mg twice a day with DPX-Survivac Vaccine and cyclophosphamide in ovarian cancer. The subject was receiving multiple medicines including alprazolam and ondansetron. The subject presented on study day 48 with complaints of tachycardia, tachypnea, palpitations, nausea, dizziness, confusion, shaking for the last hour with tremor and weakness in the legs, and jerky movements. The subject was also extremely thirsty and anxious. Lactated Ringer’s solution, lorazepam, and cyproheptadine were given to the subject and the symptoms were reduced within 30 minutes. The subject resumed treatment with no new symptoms reported. All four cases occurred in different clinical trials, were mild in severity, and the subjects recovered after supportive care interventions took place.
Thus, although four SS-like episodes occurred across multiple clinical studies, these episodes were confounded by other medical conditions that were mild in severity, and all events recovered after supportive care interventions took place. In addition, three of the four subjects were able to resume treatment with EPAC. None of the four reports was clinically substantiated to represent a true case of SS. In summary, the preclinical microdialysis data as well as the CNS penetration data in rats suggest that SS is unlikely following treatment with either EPAC alone or in combination with MAOIs such as linezolid. Moreover, no true cases of SS were demonstrated clinically. Based on the preclinical and clinical observations, EPAC does not appear to cause SS and the exclusion of MAOIs from clinical studies with EPAC has been lifted.
Acknowledgments
We thank Yu Li for excellent technical assistance in the bioanalysis of tryptophan concentrations in the plasma samples.
Authorship Contributions
Participated in research design: Zhang, Diamond, Yeleswaram.
Conducted experiments: Zhang, Bowman.
Performed data analysis: Zhang, Bowman, Maleski.
Wrote or contributed to the writing of the manuscript: Zhang, Bowman, Maleski, Diamond, Yeleswaram.
Footnotes
- Received August 22, 2018.
- Accepted April 19, 2019.
All authors are employees and stock holders of Incyte Corporation.
Abbreviations
- BBB
- blood-brain barrier
- CNS
- central nervous system
- CSF
- cerebrospinal fluid
- CTCAE v4.0
- common terminology criteria for adverse events v4.0
- ECF
- extracellular fluid
- EPAC
- epacadostat
- IDO1
- indoleamine 2,3-dioxygenase 1
- MAOI
- monoamine oxidase inhibitor
- SS
- serotonin syndrome
- SSRI
- selective serotonin reuptake inhibitor
- Copyright © 2019 by The American Society for Pharmacology and Experimental Therapeutics




{kind=link}
{kind=link}