


Abstract
Phytochemical-mediated modulation of P-glycoprotein (P-gp) and other drug transporters may give rise to many herb-drug interactions. Serial plasma concentration-time profiles of the P-gp substrate, digoxin, were used to determine whether supplementation with goldenseal or kava kava modified P-gp activity in vivo. Twenty healthy volunteers were randomly assigned to receive a standardized goldenseal (3210 mg daily) or kava kava (1227 mg daily) supplement for 14 days, followed by a 30-day washout period. Subjects were also randomized to receive rifampin (600 mg daily, 7 days) and clarithromycin (1000 mg daily, 7 days) as positive controls for P-gp induction and inhibition, respectively. Digoxin (Lanoxin, 0.5 mg) was administered p.o. before and at the end of each supplementation and control period. Serial digoxin plasma concentrations were obtained over 24 h and analyzed by chemiluminescent immunoassay. Comparisons of area under the curve (AUC)(0–3), AUC(0–24), Cmax, CL/F, and elimination half-life were used to assess the effects of goldenseal, kava kava, rifampin, and clarithromycin on digoxin pharmacokinetics. Rifampin produced significant reductions (p < 0.01) in AUC(0–3), AUC(0–24), CL/F, t1/2, and Cmax, whereas clarithromycin increased these parameters significantly (p < 0.01). With the exception of goldenseal's effect on Cmax (14% increase), no statistically significant effects on digoxin pharmacokinetics were observed following supplementation with either goldenseal or kava kava. When compared with rifampin and clarithromycin, supplementation with these specific formulations of goldenseal or kava kava did not appear to affect digoxin pharmacokinetics, suggesting that these supplements are not potent modulators of P-gp in vivo.
Implementation of the 1994 Dietary Supplement Health and Education Act sparked an upsurge in botanical supplement usage in the United States that continues to the present. Coincident with the influx of botanical supplements onto the marketplace are concerns regarding their interaction with conventional medications (Brazier and Levine, 2003). Herb-drug interactions may stem from the ability of various phytochemicals to modulate the activity of cytochrome P450 (P450) enzymes and/or drug transporters. The most noteworthy example to date is that of St. John's wort (Hypericum perforatum). St. John's wort reduces the effectiveness of many CYP3A4 and/or P-glycoprotein (P-gp) substrates because one of its phytochemical components, hyperforin, is a potent ligand for the orphan nuclear receptor, pregnane X receptor. Hyperforin-mediated activation of pregnane X receptor up-regulates both CYP3A4 and ABCB1, the respective genes for CYP3A4 and P-gp, leading to reduced bioavailability of many drugs administered p.o. (Dürr et al., 2000; Dresser et al., 2003).
A number of in vitro studies suggest that botanical supplements other than St. John's wort are capable of altering P450 activity (Zou et al., 2002; Foster et al., 2003; Strandell et al., 2004), yet results of human clinical studies have been less convincing. To date, only garlic oil (Gurley et al., 2002), goldenseal (Gurley et al., 2005), and possibly echinacea (Gorski et al., 2004) appear capable of significantly affecting human P450 activity in vivo. When compared with the number of reports addressing P450-mediated herb-drug interactions, relatively few clinical studies have investigated the effects of botanical supplementation on P-gp substrate disposition. Those that have been conducted focus primarily on St. John's wort and its effect on digoxin (Johne et al., 1999) or fexofenadine pharmacokinetics (Dresser et al., 2003). More recently, the effects of hawthorn (Tankanow et al., 2003), milk thistle, and black cohosh (Gurley et al., 2006) on digoxin pharmacokinetics were tested and found to be clinically insignificant. Because of the significant under-reporting of drug interactions and adverse events associated with dietary supplements, more clinical studies are needed to better evaluate the interaction potential of botanical supplements with P-gp substrates.
Other popular botanicals that may pose a risk for P-gp-mediated herb-drug interactions include goldenseal (Hydrastis canadensis) and kava kava (Piper methysticum). Goldenseal is a plant native to North America with a history of folk medicine use in the treatment of gastrointestinal disturbances, urinary disorders, hemorrhage, inflammation, and various infections. Often combined with echinacea, goldenseal-containing supplements currently rank among the top-selling botanicals in the United States. Recent in vitro studies have shown that an isoquinoline alkaloid present in goldenseal, berberine, is a substrate for P-gp (Maeng et al., 2002; Pan et al., 2002; Tsai and Tsai, 2004) that exhibits disparate modulatory effects on P-gp-mediated drug efflux (Lin et al., 1999a,b; Tsai et al., 2001; Efferth et al., 2002; He and Liu, 2002; Maeng et al., 2002). Kava kava has long been a traditional beverage consumed among South Pacific islanders to imbue psychotropic, hypnotic, and anxiolytic effects (Ulbricht et al., 2005). Since the 1990s, commercial kava extracts formulated as tablets and/or capsules have been marketed as dietary supplements for the alleviation of stress, anxiety, or insomnia (Côté et al., 2004; Ulbricht et al., 2005). The kavalactones (kavain, dihydrokavain, methysticin, dihydromethysticin, yangonin, and desmethoxyyangonin), a collection of phytochemicals unique to kava, have also been shown to modulate P-gp activity in vitro (Mathews et al., 2005; Weiss et al., 2005).
In this report we describe, for the first time in humans, the effects of goldenseal and kava kava supplementation on the pharmacokinetics of digoxin, a putative P-gp substrate that does not undergo extensive presystemic metabolism and exhibits a narrow therapeutic index. In addition, we compare supplement effects with those of rifampin, an inducer of P-gp expression (Greiner et al., 1999), and clarithromycin, an inhibitor of P-gp activity (Rengelshausen et al., 2003), as a means of gauging the clinical relevancy of supplement-mediated interactions.
Materials and Methods
Study Subjects. This study protocol was approved by the University of Arkansas for Medical Sciences Human Research Advisory Committee (Little Rock, AR), and all the participants provided written informed consent before commencing the study. Twenty young adults (10 women) (age, mean ± S.D. = 27.3 ± 5.7 years; weight, 77.3 ± 17.7 kg) participated in the study, and all the subjects were in good health as indicated by medical history, routine physical examination, electrocardiography, and clinical laboratory testing. All the subjects were nonsmokers, ate a normal diet, were not users of botanical dietary supplements, and were not taking prescription (including oral contraceptives) or nonprescription medications. All the female subjects had a negative pregnancy test at baseline. All the subjects were instructed to abstain from alcohol, caffeine, fruit juices, cruciferous vegetables, and charbroiled meat throughout each 2-week phase of the study. Adherence to these restrictions was further emphasized 5 days before digoxin administration. Subjects were also instructed to refrain from taking prescription and nonprescription medications during supplementation periods, and any medication use during this time was documented. Documentation of compliance to these restrictions was achieved through the use of a food/medication diary.
Supplements and Supplementation/Medication Regimens. The effect of goldenseal, kava kava, rifampin, and clarithromycin on digoxin pharmacokinetics was evaluated individually on four separate occasions in each subject. This was an open-label study randomized for supplementation/medication sequence. (“Supplementation/medication” refers to goldenseal, kava kava, rifampin, or clarithromycin.) Each supplementation phase (goldenseal or kava kava) lasted 14 days, whereas each medication phase (rifampin or clarithromycin) was of 7 days' duration. Each supplementation/medication phase was followed by a 30-day washout period. This randomly assigned sequence of supplementation/medication followed by washout was repeated until each subject had received all four products. Single lots of goldenseal (lot no. OI10184) and kava kava (lot no. A10062504) were purchased from Nature's Resource Products (Mission Hills, CA) and Gaia Herbs, Inc. (Brevard, NC), respectively. (Both companies are recognized leaders in the botanical supplement industry for providing products of high quality and consistency.) Rifampin (Rifadin, Aventis Pharmaceuticals, Kansas City, MO) and clarithromycin (Biaxin, Abbott Laboratories, North Chicago, IL) were used as positive controls for P-gp induction and inhibition, respectively. Product labels were followed regarding the recommended dosing of goldenseal root extract (1070 mg, three times daily, standardized to contain 24.1 mg of isoquinoline alkaloids per capsule); kava kava rhizome extract (1227 mg, three times daily, standardized to contain 75 mg of kavalactones per capsule); rifampin (300 mg, twice daily); and clarithromycin (500 mg, twice daily). Telephone and electronic mail reminders were used to facilitate compliance, and pill counts and supplementation usage records were used to verify compliance. Because of recent concerns regarding kava kava use and hepatotoxicity (Ulbricht et al., 2005), clinical liver function indices [i.e., aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transpeptidase, alkaline phosphatase, total bilirubin, direct bilirubin, and serum albumin] were monitored on days 0, 7, and 14 of both supplementation phases.
Digoxin Administration. After an overnight fast, subjects reported to the University of Arkansas for Medical Sciences General Clinical Research Center for digoxin administration and blood sampling. Before digoxin administration, subjects were weighed and questioned about their adherence to the dietary and medication restrictions. Female subjects were administered pregnancy tests, and only those with negative test results were allowed to participate. After the placement of a 20-gauge indwelling catheter into a peripheral vein of the forearm, a dose of digoxin (0.5 mg of Lanoxin, GlaxoSmithKline, Research Triangle Park, NC) was administered p.o. with 240 ml of water. Throughout the study, digoxin doses were administered 24 h before the start of each supplementation/medication phase (baseline) and again on the last day of each phase. Serial blood samples were obtained before and at 0.33, 0.67, 1, 1.5, 2, 3, 4, 6, 8, 12, and 24 h after digoxin administration. Each subject's blood pressure, heart rate, and respiration rate were monitored 1, 2, and 6 h after digoxin administration. Four hours after digoxin administration, subjects received identical meals consisting of a turkey sandwich, potato chips, carrot sticks, and water.
Determination of Digoxin Serum Concentrations. Digoxin serum concentrations were determined by an automated chemiluminescent immunoassay system (ACS:180 Digoxin, Chiron Diagnostics Corp., West Walpole, MA). Calibrations were performed in the range of 0.1 to 5.0 ng/ml. Serum concentrations greater than 5 ng/ml were diluted and reassayed. The lower limit of quantitation was 0.1 ng/ml. The interday accuracy for digoxin at 0.58, 1.77, and 3.48 ng/ml was 5.4, 3.7, and 2.9%, respectively. The interday precision for digoxin at 0.49, 0.98, and 1.97 ng/ml was 7, 6, and 2%, respectively.
Supplement Analysis. The phytochemical content of each supplement was independently analyzed for specific “marker compounds” by high-performance liquid chromatography (HPLC). Analytical standards of the isoquinoline alkaloids hydrastine and berberine, as well as the kavalactones kavain, dihydrokavain, methysticin, dihydromethysticin, yangonin, and desmethoxyyangonin, were purchased from ChromaDex, Inc. (Santa Ana, CA). For goldenseal analyses, standard solutions of hydrastine and berberine were prepared in methanol/water (50:50, v/v) covering a range of 1 to 100 μg/ml and used for quantitative purposes. Isoquinoline alkaloid content of goldenseal was quantitated using a modification of a previously published HPLC method (Abourashed and Khan, 2001). In brief, contents of 20 goldenseal capsules were weighed and placed in 100-ml volumetric flasks containing methanol/water (50:50, v/v). The contents of each vessel were agitated in an ultrasonication bath for 15 min. Aliquots of each sample were passed through a 0.45-μm syringe filter into HPLC autosampler vials. Twenty microliters was injected onto a Phenomenex Luna C18(2) column (150 × 4.6 mm, 5 μm) (Phenomenex, Torrance, CA) using a Thermo Separations Products component HPLC system (TSP, San Jose, CA). Compounds of interest were eluted isocratically with a mobile phase of acetonitrile/0.1 M phosphate buffer (27:73, v/v) at a flow of 1.8 ml/min. Column effluent was monitored by UV absorbance detection at a wavelength of 235 nm. Retention times for hydrastine and berberine were 3.3 and 5.7 min, respectively. The lower limit of quantitation for each analyte was 0.3 μg/ml. The interday accuracy and precision at 1, 10, and 50 μg/ml was <3%.
Kava kava was analyzed for kavalactones using a modification of a reversed-phase HPLC method described previously (Ganzera and Khan, 1999). In brief, standard curves of individual kavalactones, each covering a range of 2 to 100 μg/ml, were prepared in acetonitrile. Six 100-mg samples of the proprietary kava extract were placed in 50-ml volumetric flasks and brought to volume with acetonitrile. Flasks were placed in an ultrasonic water bath for 60 min. Fifty-microliter aliquots were filtered through a 0.45-μm syringe filter and placed in HPLC autosampler vials. Using a component Shimadzu (Columbia, MD) HPLC system, 5-μl aliquots were injected onto an YMC J'sphere H80-ODS column (4.6 × 250 mm, 4 μm) (YMC Inc., Milford, MA), and kavalactones were eluted isocratically with a mobile phase of acetonitrile/2-propanol/0.1% phosphate buffer (20:16:64, v/v/v) at a flow of 1.0 ml/min and a column temperature of 40°C. Column effluent was monitored by UV absorbance detection at 246 nm. Retention times for methysticin, dihydromethysticin, kavain, dihydrokavain, yangonin, and desmethoxyyangonin were 13, 14, 17.3, 19, 19.9, and 21.8 min, respectively. Standard curves were linear over the range of 2 to 100 μg/ml (R2 > 0.999). Extraction recoveries exceeded 95%, and relative standard deviations for interday accuracy and precision assessments were <4%.
Pharmacokinetic Analysis. Digoxin pharmacokinetics were determined using standard noncompartmental methods with the computer program WinNonlin (version 2.1; Pharsight, Mountain View, CA). Area under the plasma concentration time curves from 0 to 24 h [AUC(0–24)] and 0 to 3 h [AUC(0–3)] were determined by use of the trapezoidal rule. Rifampin, clarithromycin, and other P-gp modulators have significant effects on digoxin pharmacokinetics during the absorption phase (Greiner et al., 1999; Rengelshausen et al., 2003), which was the reason for evaluating AUC(0–3). The terminal elimination rate constant (ke) was calculated using the slope of the log-linear regression of the terminal elimination phase. Area under the plasma concentration versus time curve from 0 to infinity (AUC0-∞) was calculated using the log-linear trapezoidal rule up to the last measured time concentration (Clast) with extrapolation to infinity using Clast/ke. The elimination half-life was calculated as 0.693/ke. The apparent oral clearance of digoxin (CL/F) was calculated as dose/AUC0-∞. Peak digoxin concentrations (Cmax) and the times when they occurred (Tmax) were derived directly from the data.
Disintegration Tests. An absence of botanical-mediated effects on digoxin pharmacokinetics could stem from products exhibiting poor disintegration and/or dissolution characteristics. To address this concern, each product was subjected to disintegration testing as outlined in the United States Pharmacopeia (2005). The disintegration apparatus consisted of a basket-rack assembly operated at 29 to 32 cycles/min with 0.1 N HCl (37°C) as the immersion solution. One dosage unit (hard gelatin capsule) of each supplement was placed into each of the six basket assembly tubes. The time required for the complete disintegration of six dosage units was determined. This process was repeated with an additional six dosage units to ensure accuracy. Because there are no specifications for the disintegration time of the botanical supplements used in this study, the mean of six individual dosage units was taken as the disintegration time for that particular product. A product was considered completely disintegrated if the entire residue passed through the mesh screen of the test apparatus, except for capsule shell fragments, or if the remaining soft mass exhibited no palpably firm core.
Statistical Analysis. A repeated-measures analysis of variance model was fit for each pharmacokinetic parameter using SAS Proc Mixed software (SAS Institute, Inc. Cary, NC). Because presupplementation/medication and postsupplementation/medication pharmacokinetic parameters were determined in each subject for all four study phases, a covariance structure existed for measurements within subjects. Sex, supplement/medication, and supplement/medication-by-sex terms were estimated for each parameter using a Huynh-Feldt covariance structure fit. If supplement/medication-by-sex interaction terms for a specific parameter measure were significant at the 5% level, the focus of the postsupplementation/medication minus presupplementation/medication response was assessed according to sex. If the supplement/medicationby-sex interaction was not statistically significant, responses for both sexes were combined. Additionally, a power analysis was performed to estimate the ability to detect significant postsupplementation/medication minus presupplementation/medication effects. All four models obtained at least 80% power at the 5% level of significance to detect a Cohen effect size of 1.32 to 1.71 S.D. units (Cohen, 1988).
Results
All 20 subjects completed each phase of the study. Neither spontaneous reports from study participants nor their responses to questions asked by study nurses regarding supplement/medication usage revealed any serious adverse events. Two subjects exhibited elevated levels of AST (174 and 183 IU/l; normal range 0–40 IU/l) and ALT (55 and 97 IU/l; normal range 0–40 IU/l) after 14 days of goldenseal supplementation. These values returned to normal within 7 days of stopping goldenseal. No other liver function indices (e.g., γ-glutamyl transpeptidase, alkaline phosphatase, total bilirubin, direct bilirubin, and serum albumin) were affected by goldenseal. No subjects exhibited any changes in liver function tests while taking kava kava. Nausea, indigestion, and complaints of a metallic taste were frequently noted during clarithromycin phases. Mild indigestion and reddish discoloration of the urine were common conditions reported with rifampin use. No clinically significant changes in blood pressure, heart rate, or respiratory rate were observed after digoxin administration. Examination of pill counts and food/medication diaries revealed no significant deviations from the study protocol.
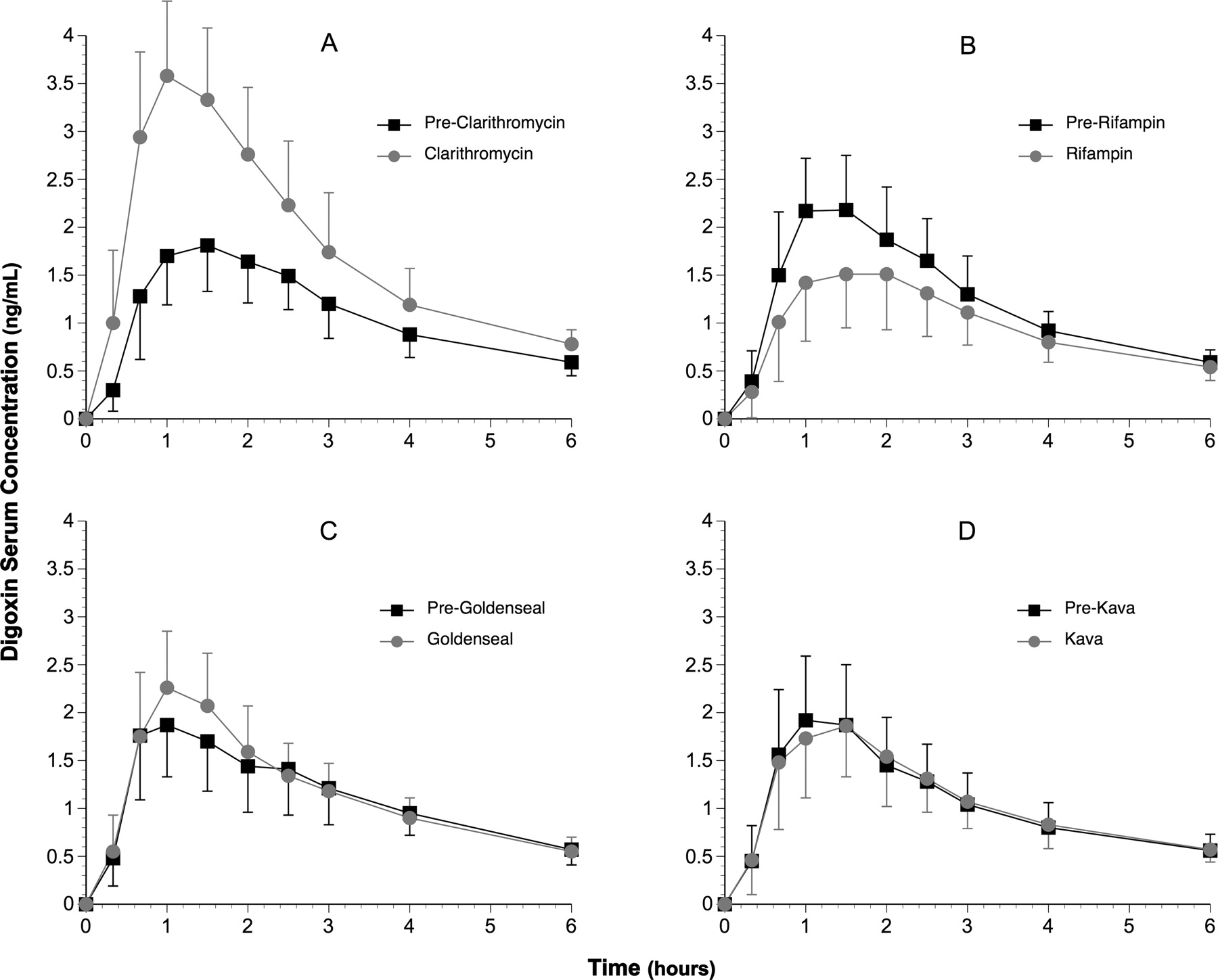
The effects of clarithromycin, rifampin, goldenseal, and kava kava on serum digoxin concentration versus time profiles are depicted in Fig. 1. Statistically significant increases (p < 0.001) in digoxin AUC(0–24) (57%), AUC(0–3) (83%), Cmax (95%), and elimination half-life (79%) were observed after 7 days of clarithromycin ingestion (Fig. 1; Table 1). Clarithromycin produced a 53% decrease in digoxin CL/F (p < 0.001) (Table 1). Statistically significant reductions (p < 0.05) in digoxin AUC(0–24) (–16%), AUC(0–3) (–27%), and Cmax (–28%) were noted following rifampin administration (Fig. 1; Table 1). Rifampin increased the CL/F of digoxin by 33% and reduced digoxin elimination half-life by 16%. Apart from a 14% increase in digoxin Cmax following goldenseal, no other significant changes in digoxin pharmacokinetics were observed as a result of goldenseal or kava kava supplementation (Fig. 1; Table 1). Digoxin Tmax was not significantly affected by any of the treatments. In addition, no sex-related changes in digoxin pharmacokinetics were noted for any of the supplement/medication interventions.
Digoxin pharmacokinetic parameters before and after supplementation/drug phases (mean ± S.D.)
Results of phytochemical analyses and disintegration testing for goldenseal and kava are presented in Table 2.
Phytochemical analysis and disintegration times for botanical dosage forms
Discussion
Considerable evidence points to the goldenseal alkaloid berberine and the kavalactones as being substrates for P-gp. After p.o. administration in the rat, berberine undergoes hepatobiliary excretion, the magnitude of which is altered by P-gp inhibitors (Tsai and Tsai, 2004). Also, using a rat recirculating intestinal perfusion model and in vitro transport systems, berberine absorption was significantly improved in the presence of the P-gp inhibitors cyclosporine and quinidine (Pan et al., 2002). Accordingly, some authors have proposed that P-gp-mediated intestinal efflux may explain berberine's poor oral bioavailability (Sheng et al., 1993; Zeng and Zeng, 1999). Still other in vitro studies point to berberine as a weak to moderate inhibitor of various P-gp substrates (Tsai et al., 2001; Efferth et al., 2002; He and Liu, 2002). Conversely, berberine has also been shown to induce P-gp expression in various cell lines (Lin et al., 1999a,b; Maeng et al., 2002).
Like berberine, studies investigating the effects of kavalactones on P-gp function in vitro have yielded mixed results. Using the P-gp-overexpressing murine leukemia cell line P388/dx, Weiss et al. (2005) showed that individual kavalactones were moderately inhibitory toward the P-gp-mediated efflux of calcein-acetoxymethylester, whereas crude kava extracts appeared to be more potent inhibitors. Of the individual kavalactones tested, desmethoxyyangonin was the most potent; however, it was 9 times less inhibitory than quinidine and 28.5 times less potent than verapamil. In contrast, studies using a baculovirus expression system showed that human P-gp ATPase activity increased 2-fold following incubation with desmethoxyyangonin but was unaffected by kava extract or other individual kava lactones (Matthews et al., 2005).

Digoxin concentration-time profiles (0–6 h) before and after each supplementation/drug phase. Pre- and post-clarithromycin (A), pre- and post-rifampin (B); pre- and post-goldenseal (C); and pre- and post-kava kava (D). Black squares = pre-experimental mean serum digoxin concentrations. Gray circles = post-experimental mean serum digoxin concentrations. Error bars = S.D.
Despite ample evidence for goldenseal alkaloids and kavalactones as modifiers of P-gp activity in vitro, our findings suggest that the goldenseal and kava formulations investigated in this study were not potent modulators of human P-gp activity in vivo and therefore do not pose a significant interaction risk with digoxin. This interpretation is supported by the significant changes in digoxin pharmacokinetics observed following the administration of clarithromycin, a known P-gp inhibitor, and rifampin, a recognized inducer of P-gp expression. The slight, albeit statistically significant, increase (14%) in digoxin Cmax by goldenseal could be interpreted as P-gp inhibition; however, when compared with clarithromycin's effect on Cmax (+95%), this is not likely to be clinically significant.
Because plasma concentrations of berberine, hydrastine, and the kavalactones were not measured, their in vivo solubility and/or bioavailability status in this study remains unknown. To date, no assessment of the pharmacokinetics of goldenseal alkaloids, when administered as a dietary supplement, has been performed in humans. However, when congestive heart failure patients received 1.2 g/day of berberine hydrochloride p.o. for 14 days, peak steady-state plasma concentrations were less than 20 ng/ml (Zeng and Zeng, 1999), signifying poor bioavailability. Whether this is a function of inadequate dissolution, extensive drug efflux, extensive biotransformation, or a combination remains to be determined.
Little is known about kavalactone disposition in humans. Duffield et al. (1989) noted that all seven major and several minor kavalactones could be identified in the urine of male volunteers after ingesting a traditional aqueous extraction of kava. The pharmacokinetic profile of kavain has also been studied in humans following its p.o. administration. An 800-mg dose of racemic kavain produced free serum concentrations of 40 and 10 ng/ml at 1 and 4 h, respectively. Higher concentrations of kavain metabolites, both free and conjugated, were noted in serum and urine, indicative of significant biotransformation.
From the available data it appears that concentrations in excess of 10 to 30 μM of either goldenseal alkaloids or kavalactones are required to significantly modify P-gp activity in vitro. Clearly, plasma levels < 20 ng/ml are unlikely to cause significant modulation of the transporter in vivo. However, following application p.o., the concentration of goldenseal alkaloids and kavalactones might be considerably higher in the gut wall. Assuming that the phytochemical contents determined for these two formulations (Table 2) are consumed with a 240-ml volume of beverage, a rough estimation of the concentrations of goldenseal alkaloids and kavalactones, assuming complete dissolution, yields concentration ranges of 157 to 240 and 132 to 417 μM, respectively. From in vitro predictions, such concentrations should be sufficient to modulate P-gp activity within intestinal enterocytes. Our findings contradict these predictions and show that extrapolation of in vitro results to the in vivo situation remains speculative. Lack of correlation between in vitro and in vivo studies with botanical extracts is not unexpected given the myriad limitations recognized for in vitro models as predictors of drug interactions in vivo (von Moltke et al., 1998). Often, such discrepancies can be traced to basic pharmaceutics issues, including inadequate dosage form disintegration and/or dissolution. In this study, however, both dosage forms disintegrated within 12 min or less, leaving phytochemical solubility concerns and poor dissolution characteristics as more plausible rationales. Indeed, berberine, hydrastine, and the kavalactones exhibit poor water solubility, a problem often addressed during in vitro studies through the addition of cosolvents like methanol or dimethyl sulfoxide. Thus, it seems reasonable to suspect that although goldenseal alkaloids and kavalactones may be P-gp substrates, they either exhibit a weak affinity for the transporter or concentrations achieved in vivo are insufficient to affect digoxin efflux.
Nevertheless, we recently reported that goldenseal supplementation inhibited human CYP3A4 and CYP2D6 activity in vivo, whereas kava kava administration had no noticeable effect on these isoforms (Gurley et al., 2005). Evidently, the concentration of certain goldenseal components is sufficient to inactivate these enzymes in vivo. This inactivation by goldenseal likely stems from the formation of a stable heme adduct between the methylenedioxyphenyl moiety of berberine and hydrastine and the heme iron of the enzyme (Chatterjee and Franklin, 2003). Interestingly, two kavalactones, methysticin and dihydromethysticin, are also substituted methylenedioxyphenyl compounds, yet they do not inhibit CYP3A4 or CYP2D6 in vivo. This may be the result of shorter, more flexible side chains attached to these methylenedioxyphenyl compounds because such substitutions are less inhibitory to P450 isoforms (Nakajima et al., 1999). Considerable overlap in the substrate selectivity, tissue localization, and coinducibility of CYP3A4 and P-gp underscores the importance of assessing the effects of goldenseal and kava kava on human P-gp activity in vivo. The appropriateness of such an investigation was heightened by a recent report citing markedly elevated blood concentrations of cyclosporine (a CYP3A4 and P-gp substrate) in renal transplant recipients after berberine administration (Wu et al., 2005). In light of our current findings, it would appear that goldenseal's mechanism for producing herb-drug interactions lies more with its ability to inhibit P450 isoforms than its effect on P-gp. Kava, on the other hand, appears to have little effect on either in vivo.
Product variability may also contribute to the observed discrepancies, not only with regard to vitro/in vivo comparisons but also among clinical studies. Commercially available goldenseal and kava formulations have been found to vary widely in their alkaloid content (Ganzera and Khan, 1999; Edwards and Draper, 2003; Côté et al., 2004). To date, no reports have examined the dissolution or phytochemical release characteristics of goldenseal or kava supplement formulations. Such information, especially that garnered from tests performed in simulated gastric or intestinal fluid, may be especially useful in explaining these inconsistencies.
Recent reports linking kava use to liver toxicity prompted its withdrawal in Europe, Australia, and Canada (Ulbricht et al., 2005). In the United States, the Food and Drug Administration issued a warning to consumers alerting them to possible hepatotoxic side effects associated with kava supplementation (Ulbricht et al., 2005). We observed no clinical evidence of kava-related hepatoxicity; however, moderate elevations in serum AST and ALT were noted in two subjects during the 14-day goldenseal supplementation period. This observation brings into question the safety of chronic goldenseal supplementation.
In conclusion, when compared with rifampin and clarithromycin, the botanical supplements goldenseal and kava kava produced no significant changes in the disposition of digoxin, a clinically recognized P-gp substrate with a narrow therapeutic index. Accordingly, these supplements appear to pose no clinically significant risk for P-gp-mediated herb-drug interactions. However, given the interproduct variability in phytochemical content and potency among botanical supplements, these results may not extend to regimens using higher dosages, longer supplementation periods, or products with improved dissolution and/or bioavailability characteristics.
Footnotes
-
This work is supported by the National Institutes of Health/National Institute of General Medical Sciences under Grant R01 GM71322 and by National Institutes of Health/National Center for Research Resources to the General Clinical Research Center of the University of Arkansas for Medical Sciences under Grant M01 RR14288.
-
Article, publication date, and citation information can be found at http://dmd.aspetjournals.org.
-
doi:10.1124/dmd.106.012708.
-
ABBREVIATIONS: P450, cytochrome P450; P-gp, P-glycoprotein; AST, aspartate aminotransferase; ALT, alanine aminotransferase; HPLC, high-performance liquid chromatography; AUC, area under the curve; ke, elimination rate constant; CL/F, apparent oral clearance.
- Received September 1, 2006.
- Accepted October 27, 2006.
- The American Society for Pharmacology and Experimental Therapeutics




{kind=link}